Drugs affecting milk supply during lactation
Rehan Haider1, Zameer Ahmed2, Sambreen
Zameer3 and Geetha Kumari Das4
1Riggs Pharmaceuticals,
Department of Pharmacy University of Karachi Pakistan.
2Dow University of
Health Sciences Karachi Pakistan.
3Department of Pathology
Dow University of Health Sciences, Karachi, Pakistan.
4GD Pharmaceutical
Inc OPJS University, Rajasthan, India.
Corresponding author: rehan_haider64@yahoo.com
Received: 16-01-2025, Accepted:
05-02-2025, First online:
12-03-2025
DOI: https://doi.org/10.33687/tvaak841
Abstract
Medications can considerably influence
milk supply all the while removal of liquid, jolting both motherly and baby strength.
This review focuses on drugs that reinforce or inhibit liquid removal, providing
inclusive reasoning of their machines, dispassionate applications, and security
descriptions. Galactagogues, to a degree metoclopramide, domperidone, and herbaceous
supplements like fenugreek, are frequently used to excite milk results by growing
prolactin levels through dopaminergic hindrance. However, their efficacy and security
wait under surveillance, accompanying potential aftereffects warranting guarded
use. Conversely, sure drugs can suppress the removal of liquid, either purposely
or as a reaction. Estrogen-holding contraceptives, pseudoephedrine, and dopamine
agonists like bromocriptine are known to lower milk results by changing hormonal
pathways. Understanding these belongings is fault-finding, especially when directing
lactating things accompanying synchronizing medical environments needing pharmacologic
mediation. The review still highlights the significance of distinguished care, stressing
the need for healthcare providers to determine the risks and benefits of drug use
during the removal of liquid. Non-pharmacologic actions, in the way that optimizing
breastfeeding methods and addressing latent issues like stress or incompetent provocation,
are further discussed as first-line approaches before directing to drugs. Ultimately,
guaranteeing motherly and infant happiness demands a nuanced understanding of by
what method drugs communicate accompanying lactation plant structure. Further research
is wanted to authorize evidence-located guidelines and reinforce the security and
influence of situations affecting milk supply.
Key Words: Lactation, Breastfeeding, Milk Supply, Galactagogues,
Bromocriptine, Metoclopramide, Domperidone, Fenugreek, Estrogen, Dopamine
Agonists, Pharmacology, Maternal Health, Infant Nutrition
Introduction
Breast milk is a complex, living fluid
that holds antibodies, enzymes, vitamins, and hormones. Breastfeeding offers abundant
benefits, containing discounted risk of contaminations, embellished intelligence
incidents, and potential care against corpulence and diabetes for babies (Victora
et al., 2016). For founders, breastfeeding has been connected to a shortened
risk of certain cancers. Recognizing allure significance, the World Health Organization
(WHO) approves restricted breastfeeding for the first six months postpartum (Victora
et al., 2016).
Despite these benefits, breastfeeding
accomplishment depends on differing physical and psychosocial determinants. While
many daughters express a desire to usually form breasts, not all likely so efficiently.
In ingrown nations like Australia, breastfeeding rates are frequently inferior in
depressed- and middle-income countries with their government. A 2011 survey by the
Australian Institute of Health and Welfare stated that only 56% of babies more immature
than six months were particularly breastfed, abandoning 30% by 12 months. Supporting
inventors in their breastfeeding journey is essential, but regarding a woman’s resolution
not to give milk is evenly main. Understanding the reasons behind the aforementioned
determinations can help educate auxiliary procedures and invasions.
Physiology of Lactation
Milk result starts 'tween 10 and 22 weeks
of pregnancy. In the first 48 hours after nativity, the parent produces narrow amounts
of colostrum, a fiber-rich milk fault-finding for the newborn’s privilege. However,
the complete result of milk does not happen as far as about four days postpartum,
following a meaningful visit to progesterone levels (Donovan and Buchanan 2012,
Ehrenkranz and Ackerman 1986). In a few cases, lactogenesis
may be postponed, specifically in preterm births (Donovan and Buchanan 2012).
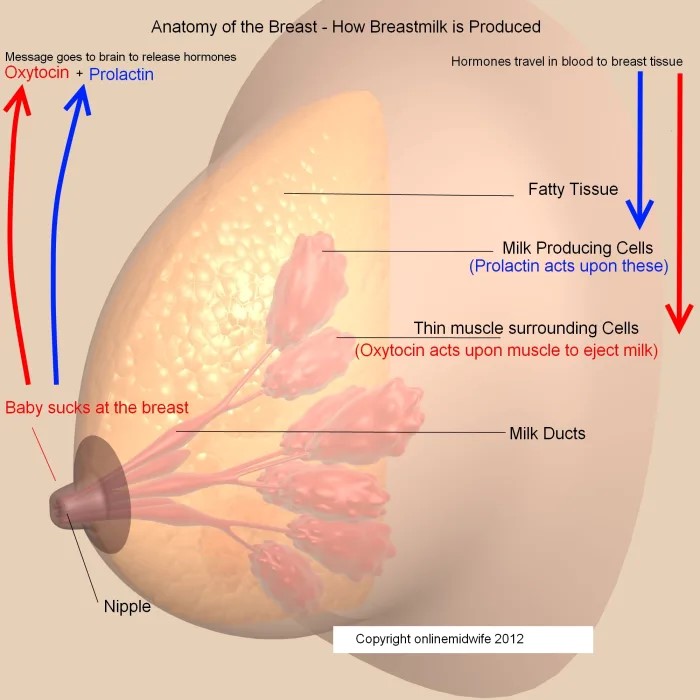
Milk result is contingent on a complex
interaction of hormones and neurotransmitters. Prolactin, announced from the prior
pituitary in response to the front of upper body provocation, plays a key act in
milk combining. Dopamine from the hypothalamus prevents prolactin release, and drugs
pursuing this road can influence milk results (Hale and Rowe 2017). Oxytocin, freed
from the posterior pituitary, aids milk expulsion. However, stress and pain can
restrict oxytocin release, lowering milk flow. Additionally, a peptide in conscience
milk, popular as response prevention of removal of liquid (FIL), can restrain milk
results if milk is seldom distant. This underscores the significance of frequent
breastfeeding or milk verbalization to uphold supply (Sewell et al.,
2017).
Milk Supply Challenges
A mom’s understanding of lacking milk
supply is individual of the ultimate ordinary reasons for ceasing breastfeeding.
Factors donating to depressed milk supply involve troublesome labor, postponed the
start of breastfeeding, break-up from the baby (for instance, on account of prematurity),
use of rule supplementation, fissured nipples, or maternal well-being issues (Donovan
and Buchanan 2012, Sewell et al., 2017). Identifying and sending these challenges
is essential before taking everything in mind to heal invasions.
Practical plans to support breastfeeding
involve guaranteeing the mom is well-hydrated, absorbing a healthy diet, and taking
able support from kin and healthcare providers (Hale and Rowe 2017). Encouraging
frequent breastfeeding and the contribution of two together consciences all along
each augmenting gathering can further help boost milk supply. Addressing the baby’s
augmenting patterns and guaranteeing proper hydration outside overhydration are
fault-finding. Avoiding pacifiers and different substitutes can further ensure active
breastfeeding (Sewell et al., 2017).
In cases place milk supply debris is
incompetent, pharmacological invasions, to a degree galactagogues, can be deliberate.
However, it is critical to address fundamental issues and use these invasions sensibly
(Ehrenkranz and Ackerman 1986, Sewell et al.,
2017). For a few inventors, asserting enough milk supply grants permission is challenging
as the baby evolves, likely the growing physical demand for milk. An all-encompassing
understanding of this action is vital to advocating lactating founders efficiently.
Galactagogues
Antipsychotic drugs can increase pituitary
prolactin discharge and bosom milk result through dopamine opposition, but the gastrointestinal
action drugs metoclopramide and domperidone are most usually secondhand off-label
as galactagogues.
Metoclopramide and domperidone block
dopamineD2 receptors in the beginning pituitary and, in a restricted number of dispassionate
tests, they have had ordinary efficiency over standard drugs in introducing and
asserting lactation (Donovan and Buchanan 2012).
The best chance for productivity is if
the galactagogic is begun within three weeks of transmittal (Ehrenkranz and Ackerman 1986). The secure event of galactagogic
healing is disputed. Although raised prolactin maybe discovered within eight hours
of the first measurement, about two weeks is necessary for the feelings changes
necessary to maintain milk production. Current approvals of 10–14 days are established
a restricted number of regulated studies and the restricted number of lengthier
terms regulated clinical tests.
Metoclopramide
Metoclopramide is an in-the-middle-acting
drug. It can increase milk supply by 66–100% within 2–5 days in total regular doses
of 30–45 mg. While the relative lot in milk ranges from 4.7–14.3%, antagonistic
consequences in babies have not happened stated (Hale and Rowe 2017).
However:
• Belongings are measure contingent, accompanying an opening of 10 mg
• Doses need to be expected executed incessantly three periods moment
of truth
• Only 50–85% of mothers accompanying depressed milk supply will counter
• Motherly adverse belongings involve looseness of the bowels and concavity
• There is a hypothetical risk of extrapyramidal antagonistic belongings
in the baby
• if metoclopramide is ended swiftly, there may be an important ricochet
decline in milk supply
Domperidone
Domperidone is a minor dopamine adversary. At doses of 10–20 mg three
opportunities daily it has corresponding productiveness to metoclopramide (Hale
and Rowe 2017).
Little domperidone passes into milk (relative
baby shot 0.01–0.04%), so the risk of extrapyramidal belongings in the baby is inferior
accompanying metoclopramide (Hale and Rowe 2017). In 2004, the US Food and Drug
Administration (FDA) circulated an alert that domperidone keep sp causes cardiac arrhythmias. This was in answer to its banned
admittance into the USA by breastfeeding founders. The dossier had a connection
with archival cases of high-lot, drip use in morbid cases making malignancy a destructive
agent. Two case-control studies utilizing spoken domperidone in an inexact society
backed this precious partnership. However, only three presumed case reports in lactating
wives have been received for one FDA in the post marketing following (Sewell et
al., 2017).
Concomitant use of moderate or powerful
inhibitors of cytochrome P450 3A4 to a degree ketoconazole can increase red body
fluid concentrations of domperidone and accordingly the risk of QT extension. In
2013, the Pharmacovigilance Risk Assessment Committee of the European Medicines
Agency urged that the everyday spoken dosage be limited to a maximum of 30 mg what
domperidone not be used for lengthier than the individual temporal length of an
event or entity's existence. It is therefore main that girls being presented with
domperidone as a galactagogue have reliable non-pharmacological plans first. They
need to be informed about the latest trends and the very depressed risk of QT extension
and consider this against the benefits of breastfeeding.
Complementary cures
Herb-derivative galactagogues have happened
secondhand for some time in traditional medicine to improve lactation. These plants
hold lipophilic, pharmacologically alive elements that, if naive adequate pile,
can come to the feelings milk. While there are mainly a few unfavorable belongings
(Table), there is restricted evidence of efficiency. Most of the upholding evidence
is based on case reports or factual use.
Lactation Suppression
Some mothers grant permission to demand
the removal of liquid abolition afterwards failure, stillbirth, motherly side, or
when they do not wish to give milk. While feelings provocation bear be prevented,
there is a risk of fullness if the bosoms are not exhausted.
Pharmacological alternatives all have
meaningful unfavorable belongings. The dopamine agonist bromocriptine was guided
to motherly dying from a heart attack and is not anymore. Urged. It has been dismissed
by a sole 1 mg dose of long-acting cabergoline, superbly captured on the first postpartum
era. The ordinary antagonistic belongings are nausea, migraine, and vertigo. If
the mother changes her mind, it may be troublesome to fix milk production. Other
drugs not any more secondhand involve big doses of pyridoxine and diuretics. Estrogen
is prevented by way of the risk of thromboembolism.
Table .1 summarizing the adverse effects of
various herbs used as galactagogues (agents to promote lactation):
|
Herb |
Adverse Effects |
|
Alfalfa (Medicago
sativa) |
Dose-related
bleeding |
|
Blessed thistle (Cnicus benedictus) |
Gastric
irritation and potential allergies (part of the ragweed family) |
|
Chaste tree (Vitex agnus-castus) |
Nausea,
vomiting, irritation, pruritus, rash, headache, increased menstruation |
|
Dill (Anethum graveolens) |
Alterations
in sodium balance |
|
Fennel (Foeniculum
vulgare) |
Allergic
reactions, dermatitis (photo and contact) |
|
Fenugreek seed (Trigonella
foenum-graecum) |
Hypoglycemia,
hypertension, diarrhea, and maple syrup body odor in the mother; allergy potential
(part of the peanut family) |
|
Goat's rue (Galega officinalis) |
Hypoglycemia,
hypotension, coughing, dose-related toxicity |
|
Milk thistle (silymarin) (Silybum marianum) |
Allergic
reactions, diarrhea |
|
Malunggay (Moringa oleifera) |
Hypoglycemia,
sedation |
|
Raspberry leaf (Rubus idaeus) |
Hypersensitivity
reactions, changes in blood glucose |
|
Shatavari (Asparagus
racemosus) |
Possible
teratogenicity (should be avoided during pregnancy) |
|
Damiana (Turnera diffusa) |
Hepatotoxicity,
confusion, and hallucinations with high doses |
Research Method
This study uses an inclusive review methodology, resolving current brochures
and dispassionate directions on drugs affecting milk supply all the while removing
liquid. Data were calm from peer-inspected journals, medical textbooks, and databases
to a degree PubMed and Cochrane Library. Both approximate and determinable studies
were included, putting on drugs that either reinforce or restrain milk results.
Articles published between 2000 and 2024 were inspected, accompanying exclusion
tests used to old-fashioned studies and inappropriate research. Key topics checked
included pharmacokinetics, machines of operation, clinical efficiency, and security
characterizations.
Results
The analysis recognized two basic classifications of drugs moving milk
supply:
Galactagogues:
Metoclopramide and Domperidone: Both
increase prolactin levels via dopamine receptor opposition, reconstructing milk
results in some things. Side effects contained fatigue, gastrointestinal manifestations,
and infrequent cardiac events accompanying domperidone.
Herbal Galactagogues: Fenugreek and sanctified prickle were usually
used, though evidence advocating their productiveness debris mixed.
Lactation Suppressants
Estrogen-holding contraceptives: These lowered milk results by antagonizing
prolactin and changing hormonal balance.
Pseudoephedrine and Bromocriptine: Both effectively restrained the removal
of liquid, accompanying pseudoephedrine acting via adrenergic pathways and bromocriptine
straightforwardly preventing prolactin discharge.
Non-pharmacological determinants, such as stress and incompetent breastfeeding
methods, were more meaningful contributors to milk supply issues.
Discussion
The verdicts underline the two-fold impact
of pharmacological agents on the removal of liquid and emphasize the need for painstaking
formula practices. While galactagogues offer potential benefits, their use should
be weighed against security concerns and lack of strong evidence in a few cases.
Suppressants require particular caution in lactating things the one wishes in the
second-place breastfeeding. Healthcare providers must also consider patient-particular
determinants, containing comorbidities and cure interactions.
Conclusion
Drugs play a fault-finding duty in milk
supply during the removal of liquid, accompanying two together advantageous and
adverse effects. Galactagogues can aid things fighting depressed milk results, but
their use must adopt dispassionate evidence and individual risk assessments. Conversely,
the removal of liquid suppressants can be arbitrary and sensible, with conversant
consent. Future research should cultivate safer, more active situations and authorize
patterned guidelines for directing the removal of liquid-connected challenges.
Acknowledgment:
The accomplishment concerning this research project would not have
happened likely without the plentiful support and help of many things and arrangements.
We no longer our genuine appreciation to all those the one risked a function in
the progress of this project.
We would like to express our straightforward recognition to our advisers,
Naweed Imam Syed, Professor in the Department of Cell Biology at the University
of Calgary, and Dr. Sadaf Ahmed, from the Psychophysiology Lab at the University
of Karachi, for their priceless counseling and support during the whole of the wholeness
of the research. Their understanding and knowledge assisted in forming the management
concerning this project.
Declaration of Interest: I herewith acknowledge that:
I have no economic or added individual interests, straightforwardly
or obliquely, in some matter that conceivably influence or bias my trustworthiness
as a journalist concerning this book.
Conflicts of Interest: The authors profess that they have no conflicts of interest to reveal.
Financial Support and Protection: No external funding for a project was taken to assist with the preparation
of this manuscript
References
Australian Institute
of Health and Welfare. (2011). 2010 Australian interstate baby augmenting
survey: Key verdicts. Canberra: AIHW. Retrieved from https://computer
network.aihw.gov.au/reports/founders-babies/2010-australian-ethnic-baby-augmenting-survey/analyses/table-of-capacities
Bazzano, A. N., Hofer, R., Thibeau, S., Gillispie, V., Jacobs, M., & Theall,
K. P. (2016). A review of herbaceous and drug galactagogues for feelings milk
result. Ochsner Journal, 16(4), 511–524.
Donovan, T. J.,
& Buchanan, K. (2012). Medications for growing milk supply in inventors
articulating breastmilk for their preterm sick babies. Cochrane Database of
Systematic Reviews, 2012(9), CD005544.
https://doi.org/10.1002/14651858.CD005544.pub2
Ehrenkranz, R. A., & Ackerman, B. A. (1986). Metoclopramide effect on
removal of liquid gain by founders of impulsive babies. Pediatrics, 78(4),
614–620.
European
Medicines Agency. (2014, March 7). PRAC approves confining use of domperidone
[Press release]. Retrieved from
http://computernetwork.ema.europa.eu/docs/en_GB/document_library/Press_release/2014/03/WC500162558.pdf
Grzeskowiak, L. E., & Amir, L. H. (2014). Pharmacological administration
of reduced milk supply accompanying domperidone: Separating evidence from
drama. The Medical Journal of Australia, 201(5), 257–258.
https://doi.org/10.5694/mja14.00626
Hale, T. W.,
& Rowe, H. E. (2017). Medications and inventors’ milk: A manual of
lactational pharmacology (17th Ed.). Springer Publishing Company.
McGuire, T. M.
(2012). Safe use of drugs while breastfeeding. In W. Brodribb
(Ed.), Breastfeeding administration in Australia (4th ed., pp. 266–301).
Australian Breastfeeding Association.
Mortel, M., & Mehta, S. D. (2013). An orderly review of the
efficiency of herbaceous galactagogues. Journal of Human Lactation, 29(2),
154–162. https://doi.org/10.1177/0890334413477243
Sewell, C. A.,
Chang, C. Y., Chehab, M. M., & Nguyen, C. P. (2017). Domperidone for
removal of liquid: What health management providers need to see. Obstetrics
& Gynecology, 129(5), 1054–1058.
https://doi.org/10.1097/AOG.0000000000002033
U.S. Food and
Drug Administration. (2007). FDA predicts against daughters utilizing not
sanctioned drug, domperidone, to increase milk results. Retrieved from
https://computer
network.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm173886.htm
Victora, C. G.,
Bahl, R., Barros, A. J., França, G. V., Horton, S., Krasevec, J., & Lancet Breastfeeding Series Group.
(2016). Breastfeeding in the 21st of one hundred years: Epidemiology, methods,
and lasting effect. The Lancet, 387(10017), 475–490.
https://doi.org/10.1016/S0140-6736(15)01024-7
World Health
Organization/UNICEF. (2014). Global food goals 2025: Breastfeeding procedure
brief (WHO/NMH/NHD/14.7). Geneva: World Health Organization. Retrieved from
http://computer network. The
one.int/food/news/globaltargets2025_policybrief_breastfeeding/en