Diphtheria
outbreak and associated risk factors assessment in Khyber Pakhtunkhwa, Pakistan
Wasia Ullah1,†, Abdul Nasir2,
, Muhammad Izaz3 , Rabia Rabia4
1Department of Zoology, Abdul Wali Khan University
Mardan 23300, Khyber Pakhtunkhwa, Pakistan.
2 Health Department, District Dir Upper 18000, Khyber
Pakhtunkhwa, Pakistan
3 World Health Organization District Dir Upper 18000,
Khyber Pakhtunkhwa, Pakistan
4 Department of Animal Sciences, Quaid e Azam
University, Islamabad 45320, Pakistan.
Corresponding author: Dr. Wasia Ullah Email: Wasiullah.dir@gmail.com
Received: 20-01-2025, Accepted: 05-02-2025, Published
online: 20-02-2025
DOI: https://doi.org/10.33687/xedf0s60
Abstract
Diphtheria,
a highly infectious disease that may be prevented by vaccine, is spreading and
poses a serious threat of becoming an epidemic and major public health concern
in Khyber Pakhtunkhwa, Pakistan. This study was aimed to examine the epidemic
from an epidemiological standpoint and offer management recommendations in
Khyber Pakhtunkhwa during the year 2024. Data of Diphtheria cases were
collected from Districts Health Information System (DHIS) of Health Department
Khyber Pakhtukhwa for the year 2024 reported from 28 districts of the province.
The data revealed 683 confirmed cases of diphtheria across 28 districts,
underlining the significant public health issue faced by the disease's ability
to spread rapidly. Among these, 58 cases were verified by laboratory testing,
highlighting the critical need for improved diagnostic services to detect
diphtheria rapidly and reliably. The study identifies six distinct outbreaks
verified in laboratories in Peshawar Nowshera, Charsadda, Bannu, Mardan, and
Swat, demonstrating the disease's widespread geographic reach and the need for
focused public health interventions in these locations. A higher prevalence was
identified in those over the age of five (87%). There is a substantial opportunity
to reduce and ultimately extinguish the risk of diphtheria becoming an
uncontrolled epidemic in the region by implementing a comprehensive and
multifaceted approach.
Introduction
Diphtheria is
caused by the Gram-positive Rod C. diphtheriae and is distinguished by
laryngitis, pharyngitis, or tonsillitis in the presence of an adhering membrane
in the tonsils, throat, and/or nose (WHO, 2003). Up to 25% of patients develop
myocarditis, and the condition can also impact the peripheral nervous system,
resulting in temporary paralysis (MacGregor et al., 2009). C. diphtheriae's pathogenicity is caused by an extracellular toxin,
and those with inadequate immunization or insufficient antitoxin antibody
levels are more vulnerable to infection (WHO, 2006). Diphtheria is treated with
antitoxin and either penicillin or erythromycin, while DAT is not currently
widely available in Nigeria (Sadoh and Sadoh, 2011).
The advent of
the diphtheria vaccination in the early twentieth century, notably the
diphtheria-tetanus-pertussis (DTP) vaccine, greatly lowered the disease's
occurrence (Rappuoli and Malito , 2014)
This historical backdrop highlights the long-standing difficulty of
diphtheria as a public health concern, which evolved from ancient descriptions
to more thorough understandings in succeeding decades. Diphtheria's history
demonstrates the enormous influence of modern advances in infectious diseases
and immunology, which have transformed it from a fearsome sickness to a
preventable condition. Although diphtheria is well controlled in many parts of
the globe because to extensive immunization, it remains a hazard, particularly
in places with insufficient vaccine coverage (Truelove et al., 2020).
Diphtheria is a highly infectious, vaccine-preventable disease. The illness is
lethal in 5-10% of instances, with a greater fatality rate in small children.
In areas with limited availability to diphtheria antitoxin, the crude fatality
rate (CFR) can reach 40% (Oduove et al.,
2024).
Despite vaccine availability, diphtheria
outbreaks continue in impoverished nations. The World Health Organization (WHO)
reported its most recent epidemic in Guinea in October 2023. A deadly
diphtheria outbreak occurred in Guinea's Kankan area between July 4 and October
13, 2023. The overall number of reported cases was 538, including 520 suspected
and 18 laboratory-confirmed cases of the illness. This epidemic resulted in 58
deaths, with 13 among the confirmed cases. This resulted in an overall case
fatality rate (CFR) of 11% across all reported cases (Zwizwai, 2023).
Notably, the demographic group most impacted by
this outbreak was children aged 1-4, accounting for the majority of infections.
Recently, an outbreak of diphtheria has occurred in one of the world's most
violent regions, Khyber-Pakhtunkhwa, Pakistan, and there is a possibility of an
epidemic as the Pakistani government makes all efforts to return Afghan
refugees to Afghanistan. This risk is worsened by the Pakistani government's
continued efforts to return Afghan refugees to Afghanistan, which might further
destabilize the already vulnerable public health situation Yousaf, 2020).
In this regard, the purpose of this study was
to conduct an epidemiological assessment of the situation and make
recommendations for how to address it. The evaluation
research considers a variety of parameters, including the demographic and
geographic distribution of cases, the incidence of infection, and the efficacy
of current public health interventions. It also examines the influence of
refugee migrations on disease transmission and identifies high-risk communities
that need rapid treatment. The outcomes of this study are critical for guiding
public health policies and interventions. Recommendations are made to
effectively address the situation, focusing on both short-term emergency
remedies and long-term prevention measures. The study also investigates the
possibility of international collaboration and aid, as the pandemic has
far-reaching consequences.
Materials and Methods
Study Area
Khyber
Pakhtunkhwa, located in northwest Pakistan, is one of the country's four
administrative provinces, despite its tiny size. It has seven divisions and 36
districts. According to the most recent census estimates, the province's
population increased from 17.7 million to 30.5 million between 1998 and 2017,
above Pakistan's overall growth rate of 2.40% by 2.89% (Wazir and Goujrn, 2021)
Predominantly rural, 81% of the population lives in the countryside,14 despite
the presence of some heavily populated towns, like Peshawar, which has 2.1
million people. Furthermore, it is anticipated that more than 3 million Afghan
refugees have arrived in the area (Braam, 2022).
Khyber
Pakhtunkhwa has seen years of assault and political uncertainty, posing
enormous economic and social development hurdles. The surge of refugees,
continued conflict, and prolonged instability have all had a negative impact on
the region's economy (Baloch et al., 2017).
Ethical Statement
Since
the study's data contained no patient identifying information, the ethical
board does not need to fully evaluate it. Before the study started, all
required consents and permissions were acquired from the data holders.
Study Design
This
study used a retrospective approach to determine the prevalence and incidence
rates of diphtheria in Khyber Pakhtunkhwa (KPK), Pakistan. The study sought to
offer a thorough assessment of the disease's impact over a certain time period
by analyzing historical data from medical records, health surveys, and regional
health department reports. The retrospective study method entailed methodically
evaluating patient records from hospitals and clinics throughout KPK, finding
verified cases of diphtheria, and collecting pertinent information such as
patient demographics, clinical features, and outcomes.
This
technique allowed the researchers to compute the prevalence rate, which
reflects the proportion of the population afflicted by diphtheria at a certain
moment in time, as well as the incidence rate, which quantifies the number of
new cases occurring during a given time period. In addition to frequency and
incidence rates, the study aimed to uncover possible risk factors for
diphtheria infection. This involved investigating characteristics such as age,
gender, socioeconomic position, immunization history, and geographic region.
Understanding these risk variables is critical for designing effective public
health interventions and disease prevention methods.
Furthermore,
the retrospective research design enabled the analysis of temporal patterns in
diphtheria cases, offering insights into how the illness has evolved in KPK.
This data is critical for assessing the efficacy of previous and current public
health interventions and identifying areas where greater efforts are required.
The study's goal is to highlight the regional burden of diphtheria by
accurately estimating prevalence and incidence rates, as well as the urgent
need for improved surveillance, vaccination campaigns, and health-care
infrastructure improvements to mitigate the impact of this potentially fatal
disease.
Results
Diphtheria
is a substantial public health hazard in Khyber Pakhtunkhwa, Pakistan, as
indicated by data gathered until December 2024. A total of 683 diphtheria cases
have been documented in 28 districts and 325 Union Councils (UCs),
demonstrating the spread of this bacterial illness. The study identified six
unique outbreaks, which were verified by lab testing, in the districts of
Peshawar (208/683, 30.45%), Nowshera (88/683, 12.88%), Charsadda (65/683,
9.51%), Bannu (53/683, 7.75%), Mardan (47/683, 6.88%), and Swat (31/683,
4.53%). (Table 1a & Figure 1b)
These
incidents highlight the disease's diverse geographical distribution and the
importance of focused public health interventions throughout the province. This
widespread geographic distribution demonstrates the disease's propensity to
afflict both urban and rural people, emphasizing the critical need for a strong
public health response. The issue is aggravated by the presence of 58
laboratory-confirmed outbreaks, which indicate localized clusters of illness
that might possibly spread to larger epidemics if early measures are not
implemented.
Table 1a:
Showing district wise detail of Diphtheria cases in Khyber Pakhtunkwha,
Pakistan
|
S. No |
District |
NO. of cases |
Percentage |
|
1 |
Peshawar |
208 |
30.45 % |
|
2 |
Nowshera |
88 |
12.88 % |
|
3 |
Charsadda |
65 |
9.51 % |
|
4 |
Bannu |
53 |
7.75 % |
|
5 |
Mardan |
47 |
6.88 % |
|
6 |
Swat |
31 |
4.53 % |
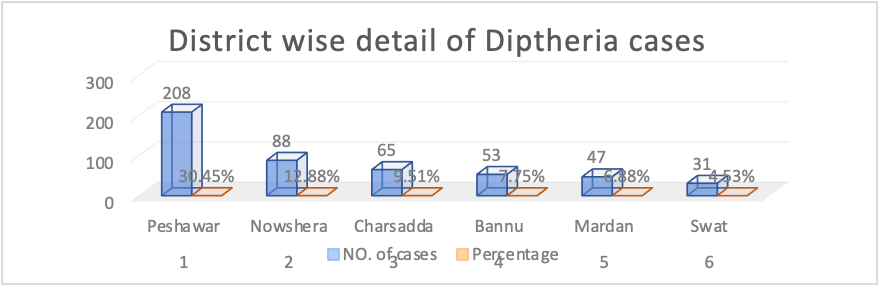 Figure 1b : Showing district wise detail of Diphtheria
cases in Khyber Pakhtunkwha, Pakistan
Figure 1b : Showing district wise detail of Diphtheria
cases in Khyber Pakhtunkwha, Pakistan
One of the most concerning characteristics of
this outbreak is the vaccination status of the afflicted people. A staggering
92% of the reported cases (n=625) were people who had no recorded history of
taking the diphtheria, pertussis, and tetanus (DPT) vaccination. This
significant figure emphasizes the importance of insufficient immunization
coverage as a primary cause of the current pandemic. Despite the global
effectiveness of immunization efforts in lowering diphtheria incidence, this
data shows considerable gaps in vaccine uptake, which might be attributed to
logistical problems, vaccine hesitation, or systemic inadequacies in the
healthcare delivery system. This situation emphasizes the importance of
prioritizing routine immunization programs while also addressing challenges to
vaccine accessibility and uptake.
The age distribution of the patients
exacerbates the problem. A considerable 87% (n=592) of the cases are recorded
in people aged five years or older, with ages ranging from 60 months to 42
years (Table 2a and Figure 2b). This
vast age range implies that diphtheria is not limited to young children, who
are commonly regarded as the major target population for DPT vaccine. Instead,
it exposes weaknesses in older age groups, which might indicate a lack of
booster doses or diminishing immunity over time. The presence of people as
elderly as 42 years old in the afflicted population suggests a probable cohort
effect, in which specific age groups missed vaccinations during previous
immunization campaigns or periods of political or social turmoil.
Table 2a:
Showing age wise detail of Diphtheria cases in Khyber Pakhtunkwha, Pakistan
|
S. NO |
Age group |
NO. of cases |
Percentage |
|
1 |
<5 years |
91 |
13 % |
|
2 |
≥5 years |
592 |
87 % |
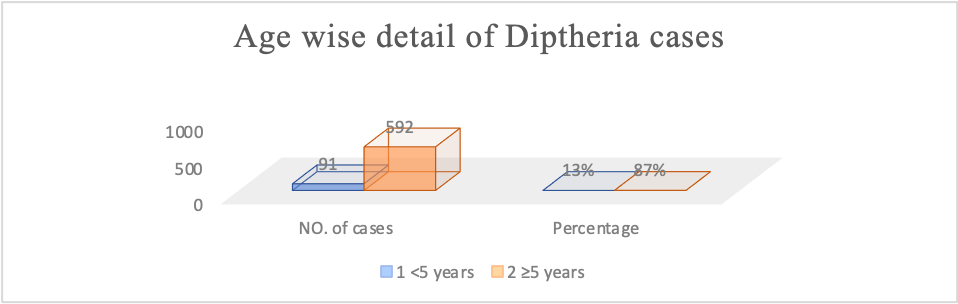 Figure 2b: Showing age wise detail of Diphtheria cases in
Khyber Pakhtunkwha, Pakistan
Figure 2b: Showing age wise detail of Diphtheria cases in
Khyber Pakhtunkwha, Pakistan
The
mortality numbers highlight the outbreak's severity. 31 diphtheria-related
deaths have been documented, resulting in a case fatality rate (CFR) of around
4.5% in 2024. While this CFR is consistent with worldwide estimates for treated
patients, it serves as a sharp reminder of diphtheria's potentially lethal
nature, especially when prompt availability to antitoxin and supportive
treatment is restricted. The deadly consequences underline the necessity of
early detection, fast response mechanisms, and the availability of life-saving
medications in hospital settings.
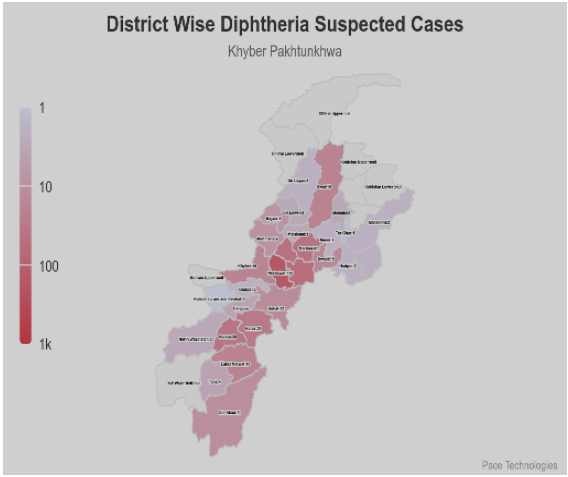
Figure 3: A choropleth map showing diphtheria cases in
various districts.
(EPI Review, 2024)
The present diphtheria outbreak demonstrates
the essential relationship between vaccination coverage, age-related
vulnerabilities, and healthcare system preparation. The significant number of
unvaccinated people and the diverse age range of afflicted patients highlight
the importance of a comprehensive public health plan. To reduce diphtheria
transmission and avoid future outbreaks, regular immunization programs must be
strengthened, booster doses made available, and disease surveillance improved.
Addressing the underlying reasons of vaccine hesitancy and raising community
understanding about the advantages of immunization will also be critical in
reducing this avoidable disease.
Discussion
The present study identifies major obstacles in
controlling infectious and non-infectious diseases in low-resource settings
like Khyber Pakhtunkhwa, Pakistan. Delayed case identification is a widespread
problem, especially for illnesses with symptoms similar to tonsillitis, where
people frequently seek medical attention at late stages (Eiseberg et al.,
2021). This delay raises the risk of misdiagnosis, contributes to greater
transmission rates, and diminishes the proportion of laboratory-confirmed cases.
As a result, illness development becomes more difficult, emphasizing the
importance of quick and precise diagnosis (Eiseberg et al., 2021; Gunning et al.,
2020; Sein et al., 2016).
Inappropriate responses to disease outbreaks,
such as diphtheria, may include focused efforts in the local or neighboring
areas, resulting in ineffective disease control. Vaccination coverage remains a
major problem, particularly among youngsters who have not gotten any doses or
have finished the whole schedule. Compliance with second-dose immunizations is
frequently challenging, particularly among adults. The prevalence of diphtheria
infections in people aged five and up calls into question long-held beliefs
that the disease affects only young children. This conclusion emphasizes the
need to revise vaccination campaign target groups and the relevance of
community-wide immunity in protecting all ages (Siegel et al., 2018).The
diverse age range of those afflicted, ranging from babies to the elderly,
emphasizes the general sensitivity to diphtheria in the absence of appropriate
immunization, demanding universal coverage rather than focusing primarily on
pediatric groups.
The case fatality rate (CFR) of 5%, which
equates to 16 fatalities, highlights the seriousness of diphtheria and its
preventability with efficient immunization efforts. School-age children were
identified as the most afflicted population, indicating the possibility of fast
disease spread within and between communities. Even vaccinated youngsters who
have not had booster doses remain susceptible to illness. Because of its
scarcity, anti-diphtheria serum (ADS) is difficult to get. Furthermore,
antibiotic distribution is hampered by resistance, which is frequently caused
by financial barriers and the absence of symptoms in asymptomatic carriers,
complicating attempts to prevent disease transmission. Limited district-level
resources for free antibiotics worsen the issue by extending infectious periods
and increasing transmission risks.
The provision
of prophylactic antibiotics for close contacts of confirmed patients is
critical for limiting transmission and preventing the emergence of asymptomatic
carriers (Truelove et al., 2020). Implementing successful control measures
requires coordinated efforts from public health authorities, healthcare
providers, and the community. Public awareness efforts must highlight the
significance of timely immunization and early treatment seeking behavior.
Collaboration with international health organizations can offer the technical
and financial assistance needed to boost diphtheria control efforts in the
region (Pagliusi et al., 2019). The
persistent threat of vaccine-preventable illnesses in Khyber Pakhtunkhwa
emphasizes the importance of monitoring and aggressive public health
initiatives.
The terrible loss of 16 lives due to a
preventable illness highlights the importance of improving public health
measures. Strategies to strengthen vaccine supply chains, raise immunization
awareness, and extend outreach initiatives to underprivileged populations are
critical for reducing the danger of future outbreaks.
Diphtheria-Pertussis-Tetanus (DPT) vaccine coverage is poor, indicating
systemic inadequacies in public health infrastructure and outreach initiatives.
Factors such as vaccination accessibility, population awareness, and vaccine
reluctance all contribute to this disparity, emphasizing the need for focused
treatments.
Continuous surveillance and study are required
to better understand the dynamics of vaccine-preventable illnesses across
populations and geographies. Such initiatives can help to uncover immunization
gaps, understand disease transmission patterns, and develop targeted therapies
to meet the requirements of certain communities. Public health officials must
actively combat vaccine misinformation, which contributes considerably to
vaccine reluctance and low immunization rates. Delays in getting specialized healthcare
services not only jeopardize patient outcomes, but also promote disease spread.
Furthermore, insufficient infection prevention and control (IPC) procedures in
healthcare settings turn hospitals into potential hotspots for diphtheria
transmission.
The delayed
speed of on-the-ground investigations and response operations exacerbates the
disease's spread in impacted areas. Finally, the absence of preventive
antibiotics for close contacts is a wasted chance to break the transmission
chain successfully. To address these issues, a diversified strategy is
required, including better public health infrastructure, improved vaccination
distribution systems, extensive community participation, and long-term
international partnership. These activities are critical for averting future
epidemics and protecting public health in susceptible places.
Conclusion
The
findings highlight the importance of a comprehensive approach to address the
recurrence of diphtheria in Khyber Pakhtunkhwa. A multifaceted strategy, as
advised, is critical for strengthening the region's ability to successfully
prevent and control diphtheria epidemics. Each recommended proposal is crucial
to an overall diphtheria control strategy. Increasing immunization coverage is
critical. Adding booster doses to the Expanded Programme on Immunization (EPI)
schedule closes a crucial gap in the present immunization approach. This
strategy would assist to sustain population immunity while also protecting
against the possibility of immunity decreasing over time. Targeting all age
groups, with an emphasis on the most vulnerable demographics, is critical to
ensuring broad coverage. Another
essential proposal is to improve diagnostic and laboratory capacity.
Controlling an outbreak requires quickly and properly identifying diphtheria
cases. Improved laboratory capacity ensures rapid diagnosis, allowing health
officials to conduct targeted treatments quickly. This includes teaching health
care personnel to recognize diphtheria signs and properly manage cases, which
is critical for early diagnosis and containment.
Conflict of
Interest: The authors declare no conflict of interest
Acknowledgments.
We
are extremely thankful to the Department of Health Information System,
Government of Khyber-Pakhtunkhwa (KPK), for their tremendous assistance in
providing the required data for this study. This study could not have been
carried out and completed without their support and commitment to public health
research. We also appreciate the efforts of the staff members that allowed data
access and gave valuable insights for our work.
References
BalochA, ShahSZ, NoorZM, et al. The
economic effect of refugee crises on neighboring host countries: empirical
evidence from Pakistan. Int Migr. 2017;55(6):90–106. doi:10.1111/imig.12389.
Braam D. Zoonotic Disease Dynamics in Displacement: A Multisite Case Study
in Sindh, Pakistan and Mafraq, Jordan. University of Cambridge; 2022. doi:10.17863/CAM.96083.
Eisenberg N, Panunzi I, Wolz A, et al. Diphtheria antitoxin administration, outcomes,
and safety: response to a Diphtheria outbreak in Cox’s
Bazar, Bangladesh. Clin
Infect Dis. 2021;73(7):e1713–e1718. doi:10.1093/ cid/ciaa1718.
Gunning CE, Mwananyanda L, MacLeod WB, et al. Implementation and adherence of routine
pertussis vaccination(DTP)in a low-resource urban birth cohort. BMJ Open. 2020;10(12):e041198. doi:10.1136/bmjopen-2020-041198.
MacGregor, RR. Corynebacterium diphtheriae. In Mandell, GL, Bennett, JE, Dolin, R, eds. Mandell, Douglas, and Bennett's
Principles and Practices of Infectious Diseases, 7th edn. Philadelphia: Elsevier, 2009, pp. 2687–2693.
Oduoye MO, Marsool MDM, Haider MU,
et al. Unmasking diphtheria in Nigeria: a multifaceted approach to tackle
outbreaks and improve immunization rates among the Nigerian population—an updated correspondence. Health Sci Rep. 2024;7(1):e1804. doi:10.1002/hsr2.1804.
Pagliusi S, Che Y, Dong S. The art of partnerships for
vaccines. Vaccine. 2019;37(40):5909–5919. doi:10.1016/j.vaccine.2019.07.088.
Rappuoli R, Malito E. History
of Diphtheria Vaccine Development. In: Burkovski A, ed. Corynebacterium Diphtheriae and
Related Toxigenic Species. Springer Netherlands; 2014:225–238. doi:10.1007/978-94-007-76241_11.
Review of Expanded Program on
Immunization, Government of Khyber Pakhtunkhwa Pakistan, 31st
December, 2024.
Sadoh, AE, Sadoh, WE. Diphtheria mortality in
Nigeria: the need to stock diphtheria anti-toxin. African Journal of Clinical and Experimental Microbiology 2011; 12: 82–85.
Sein C, Tiwari T, Macneil A,
et al. Diphtheria outbreak in Lao People’s Democratic Republic, 2012–2013. Vaccine.
2016;34(36):4321–4326. doi: 10.1016/j.vaccine.2016.06.074.
Siegel JD, Guzman-Cottrill JA. Pediatric Healthcare Epidemiology. In: Principles and Practice of
Pediatric Infectious Diseases. Elsevier; 2018:10–25.
Truelove SA, Keegan LT, Moss WJ, et al. Clinical and Epidemiological Aspects of
Diphtheria: A Systematic Review and Pooled Analysis. Clin Infect Dis. 2020;71(1):89–97. doi:10.1093/cid/ciz808.
Wazir A, Goujon A. Exploratory Assessment of the Census of Pakistan Using Demographic
Analysis. J Off Stat. 2021;37(3):719–750. doi:10.2478/ jos-2021-0032.
World Health Organization.
WHO-recommended standards for surveillance of selected vaccine-preventable
diseases: May 2003 (www.who.int/vaccines-documents/).
World Health Organization. WHO position paper: diphtheria vaccine. Weekly Epidemiological Record 2006; 81: 24–31.
Yousaf F. Pakistan,
Regional Security and Conflict Resolution: The Pashtun “tribal” Areas. Routledge; 2020.
Zwizwai R. Infectious diseases surveillance
update. Lancet Infect
Dis. 2023; 23(10):e407. doi:10.1016/S1473-3099(23)00585-6