g)
SARS-CoV-2 Reinfection Rate
Infection with the
same virus had been a worrying factor, even more so with the identification of omicron
variants, which are highly infectious and can evade the immune system (Pulliam et al, 2022). Although the total reinfection
probability with different variants of the virus is around 0.94 %, it was lower,
at a level below 0.6 % until the discovery of Omicron (25). Currently, the reinfection
rate has increased to 4.1% that comes from Omicron’s multiple mutations particularly
in the spike protein that led to the lowered neutralising antibodies. Some of these
include mutation of the virus, and decline in immunity after sometime, and the fact
that the virus can overcome defences from natural infection and even the vaccines.
While vaccination, and more specifically with booster doses, and hybrid immunity
help one a degree, still, they cannot shield a person from reinfection. Higher reinfection
rates with Omicron mean that there is a question of public health, having enough
hospital beds, adapting testing and isolation measures. All these challenges point
to the need for variant-specific vaccines and constant assessment of virus evolution
in order to reduce the effects of reinfection (Chen et al., 2024).
2.
Pathogenesis
SARS-CoV-2, the virus responsible
for COVID-19, is composed of four structural proteins: cleavage and polyprotein
precursors, spike (S), envelope (E), membrane (M), and nucleocapsid (N) proteins
(Akkiz et al., 2021). Spike protein that is necessary for entering
the host cells is composed of two major structural domains, S1 and S2. The S1 domain
of the spike protein is responsible for the receptor binding and S2 domain is with
the membrane fusion of viral with host cells. In S1Domain, there is a large variation
in the Receptor Binding Domain (RBD) that further binds with the host cell receptor.
Because of the existence of similarity between SARS-CoV-2 and SARS-CoV, researchers
were able to confirm that SARS-CoV-2 requires the receptor, angiotensin-converting
enzyme 2 (ACE2) for host cell entry (Jiang et al., 2020). TMPRSS2 helps in the cleavage of the spike
protein to enhance membrane fusion and viral entry into the host cells. MERS-CoV
prefers ACE2 and these have been reported in varying density in organs such as the
lung, hear, kidneys and intestines etc and the region where the virus binds to ACE2
determines the symptoms manifested such as lung inflammation or myocarditis (Wu et al., 2020).
The initial response of the whole
organism to combat SARS-CoV-2 is inflammation. Viral entry is sensed by pattern
recognition receptors, PRR, detecting pathogen-associated molecular pattern, PAMPs
and leads to the release of pro-inflammatory cytokines such as IL-6 and chemokines
such as CCL2. IFN-1 is an important element in antiviral activity: enzymes participate
in the degradation of viral nucleic acids and proteins and perform the release of
viruses. Still, through its non-structural proteins that interfere with signalling
pathways while degrading mRNA for IFN-1, SARS-CoV-2 can suppress this response (Chen et al., 2020).
One of the grave immunopathological
reactions that occur in the course of SARS-CoV-2 disease include the cytokine storm
characterised by elevated levels of IL-6. This is a common with the Acutely Ill
clients and if not well managed; it can result in complications such as tissue damage
and organs like the heart, liver and kidneys may fail. Macrophages involvement in
cytokine storms is suggested by the direct binding of the viral spike protein to
ACE 2 receptors in the cells (Deng et al., 2017).
Regenerative immune responses
to SARS-CoV-2 consist of antibody synthesis and T-cell dependent cytolysis. CD4+
lymphocytes are involved in the humoral response and produce IgM, IgG and IgA antibodies.
The neutralizing antibodies can also specifically target the S protein or RBD without
entry into cells apart from inhibiting viral entry, it can also induce ADCV and
ADP. CD8+ lymphocytes are engaged in the destruction of the infected tissues thus
shed light on the importance of adaptive immune responses in the regulation of SARS-CoV-2
infection (Channappanavar et al 2017;
Zohar et al., 2020).
i.Infection Stage of SARS-CoV-2
SARS-CoV-2 infection
has been described in three phases according to the severity of COVID-19 it causes.
First stage is the incubation period which starts right from a time an individual
contracts the virus and the virus multiplies within the host. In this phase, people
are usually asymptomatic and there is no clinical manifestation. The second stage
is called the dissemination stage after onset of acute pneumonia and typical manifestations
of the disease, such as cough and fever (Vetter et al., 2020). In patients with chronic diseases, such
as diabetes or cardiovascular disease, this stage can be accompanied by the development
of hypoxia. In case of non-recovery, the disease goes through to the advanced third
stage that is dominated by systemic hyper inflammation. This stage can cause multiple
organ dysfunction particularly to the kidneys, liver and G.I tract (Mehta et al., 2020; Gupta et al., 2020).
Consideration of comorbidity
in COVID-19 patients was attributed to higher death incidences. Co-morbidity means
the pre-existence of another disease apart from the main disease that is diagnosed
in a patient. Symptoms of COVID-19 include fever, cough, sore throat, tiredness,
chest pain or pressure, loss of smell or taste, difficulty breathing and confusion,
muscle or joint pain, skin changes, high blood pressure, kidney problems, and diabetes
(Singh et al., 2021). They also greatly raise the risk for severe
disease and mortality, because they increase ACE2 expression, thereby vulnerability
and disease severity with SARS-CoV-2 infection. For patients with multiple comorbidity,
or multimorbidity, are at even higher risk, with mortality rates that are double
those of patients without the conditions (Agrawal et al., 2021).
ii.Long COVID
i.Definition of Long COVID
Long COVID also called
post-acute sequelae of SARS-CoV-2 infection (PASC) is a condition of ongoing symptoms,
new symptoms, or worsening symptoms occurring four weeks or later following the
initial phase of COVID-19 (Carfì et al., 2020). These symptoms may persist for anything
from weeks and months to years or even indefinitely and recipients continue to suffer
from organ dysfunction and decreased quality of life. Long COVID refers to symptomatic
COVID-19 within the 4–12 weeks’ window and beyond the initial 12 weeks. Some present
signs include; dizziness, weakness, general malaise, confusion, chest pain, joint
pain and concentration difficulties. Long COVID symptoms can persist irrespective
of the form and severity of the primary infection phase and is not limited to specific
age demography (Greenhalgh et al., 2020).
ii.Epidemiology of Long COVID
Diagnosis of long
COVID also presents a problem due to the fact that it cannot be based on one’s viral
status because most of the patients who suffer from this condition test negative
when examined with a PCR test (van et al 2019).
Recovery time also differs with each person depending on the first attack and response
to the disease. For the symptoms were never present, or at least starting from this
moment, tests for COVID-19 were not carried out, diagnosis is much more difficult.
Long COVID is thought to affect 10–30% of individuals with mild symptoms of the
disease and 50–70% of those with severe symptoms. The protected people look completely
different: out of 100 immunized patients, only 10-12 get long COVID (Ayoubkhani et al., 2022).
Long COVID is characterized
by a wide range of symptoms which affect the respiratory, gastrointestinal, neurological,
musculoskeletal, hematopoietic, and endocrine systems. Some may experience one or
more of the signs that are, tiredness, headache, and depression. Furthermore, long
COVID has overlapping characteristics with post-acute sequelae of SARS-CoV-2 infection
(PASC), including ME/CFS, during and after exertion (Singh et al., 2022).
iii.Pathogenesis of Long COVID
This is why fatigue
and hypoxia in patients with long COVID can be explained by innate SARS-CoV-2-mediated
hypercoagulation (Fogarty et al., 2021). It sparks platelet and endothelial cell
activation and causes clotting that leads to blockade of blood vessels and hence
poor tissue oxygenation. The SARS-CoV-2 viral spike protein enlarges the inflammation
signalling by activating platelets and enhancing the fibrinogen clumping resulting
in micro-clots (Grobbelaar et al., 2021). In case these micro-clots do not dissolve
through fibrinolysis, hypoxia ensues, decaying tissue function.
Mitochondrial dysfunction
is another reason people, experiencing long COVID symptoms, might be facing. There
is a strong association between disease severity and impaired mitochondrial function
in PBMCs of COVID-19 patients (Ajaz et al., 2021). This impairment affects ATP generation
which in turn affects cellular energy metabolism and as a result various symptoms
seen in long COVID.
Neurological signs
include loss of smell in patients with damage to the olfactory bulb or the olfactory
mucosa. Using MRI, investigations have evidenced that acute COVID-19 leads to stern
cell odontology, olfactory stem cells that are developed to accept ACE2 receptors
(Vaira et al., 2020). These stem cells become damaged and are
unable to help regenerate the olfactory epithelium which leads to anosmia even after
the infection has cleared. This reduced regenerative capability is the basis for
the chronic loss of sensation that can be seen in some patients.
iv.Treatments for Long COVID
There is no universal
cure for long COVID and the treatments depend on the symptoms presented by the patient
and therefore should be done clinically. Treatment involves drug therapy, counselling,
vocational rehabilitation and physiotherapy. The goal of treatment is to work with
given symptoms and try to deal with the reasons for them (Davis et al., 2023).
Preventative remains
the most effective measure – cutting the likelihood of contracting long COVID symptoms
by a highly significant extent if given prior to SARS CoV2 exposure. However, vaccination
does not cure the already existing long COVID symptoms (Watanabe et al., 2023). Various research has proved that early
vaccination will reduce the chances of developing long COVID, especially in adults.
The diabetes type
drug known as Metformin has also been seen to minimize the possibility of long COVID
in patients diagnosed with COVID-19 and comorbidity of diabetes (Mccarthy et al., 2023). Long COVID is still being researched, and
many potential treatments for patients can be found at that institution’s RECOVER
trial (Mccarthy et al., 2023). For instance, RECOVER-VITAL looks at
the use of Paxlovid for long COVID, and RECOVER-NEURO is analyzing approaches for
neurological manifestations, including online training and non-invasive brain stimulation.
Other trials planned in the future include RECOVER-SLEEP for sleep disturbances,
and RECOVER-AUTONOMIC for dysfunction of the autonomic nervous system (Zimmerman et al., 2024).
Thus, long COVID continues
to complicate what is already a burden to healthcare systems anywhere in the world.
The following should be done in order to reduce the infections, hospitalizations,
and long COVID cases which can help to ease this burden; Getting more people for
booster doses especially for the new variants.
3.
Diagnostic Methods
i.Nucleic Acid Amplification Test (NAAT)
The Nucleic Acid Amplification
Test (NAAT), which detects viral RNA and has excellent sensitivity and specificity,
is a key diagnostic tool for SARS-CoV-2 infection (Gao et al., 2021; Ravindra et al., 2021). These tests are essential for diagnosing acute COVID-19 and for tracking
the existence of the virus in people who may have chronic COVID. RT-qPCR, multiplex
RT-qPCR assays, RT-dPCR, and other cutting-edge technologies are important forms
of NAATs (Wu et al., 2020).
ii.RT-qPCR
The gold standard to detect SARS-CoV-2
infection is Real-Time Quantitative Polymerase Chain Reaction (RT-qPCR), which has
a high sensitivity and specificity (54). Through the use of reverse transcription
(RT) of viral RNA into complementary DNA (cDNA) and real-time PCR amplification,
SARS-CoV-2 RNA could be detected and evaluated. It performs most effectively in
the very initial stages of infection, when the viral load is at its highest level,
which allows prompt action to stop the virus's spread. Samples are first collected,
usually from nasopharyngeal or oropharyngeal swabs, which usually have a higher
viral load. After extracted RNA is reverse-transcribed to create cDNA, primers and
probes that target particular SARS-CoV-2 genes, including the N (nucleocapsid),
S (spike), E (envelope), and RdRp (RNA-dependent RNA polymerase) genes, are used
to amplify the cDNA. Fluorescent probes enable for real-time measurement during
amplification by releasing signals according to the amount of DNA produced. The
cycle threshold (Ct) value that RT-qPCR yields helps determine the severity of the
disease by reflecting the viral load. RT-qPCR is resource-intensive and depends
on the stage of infection, and it may produce false negative results due to poor
sample collection, low viral loads, or genetic alterations, despite its quick turnaround
time and versatility. However, RT-qPCR continues to be the mainstay of SARS-CoV-2
diagnosis, and new developments are expanding its use in pandemic management (Akkiz et al., 2021).
iii.
Multiplex RT-qPCR Assays for Detecting
SARS-CoV-2 and Other Respiratory Pathogens
SARS-CoV-2 and other
respiratory pathogens can be identified in a single reaction by multiplex RT-qPCR
tests, which are technically advanced diagnostics tools. This technique is particularly
useful in differential of COVID-19 from other viral diseases such as flu, RSV or
adenoviruses which often have similar symptoms. To identify certain genomic portions
of SARS-CoV-2, N, E or S gene or any specific genes associated with the other infections,
primers and probes are required. It is the detection of nucleotide sequences within
several targets at once at the end of which in a single reaction tube, viral RNA
isolated from a patient sample is transcribed into cDNA. Quantification and identification in real-time
are possible due to the incorporation of fluorescent labelled dyes which emit different
signals that are unique for the pathogen discovered. As a result of our study, it
can be concluded that the advantages of multiplex RT-qPCR include the increased
epidemiological activity, shorter time to diagnosis, wider possibilities of identifying
co-infections, and efficiency. However, there are drawbacks associated with this
method; assay design is complex, costs are higher and data interpretation becomes
difficult when multiple infections are present. Nevertheless, multiplex RT-qPCR
tests have been essential in the COVID-19 pandemic response as it may facilitate
faster and accurate diagnosis of respiratory diseases and enhance the care of patients
in areas that are afflicted by overbearing respiratory pathogen epidemics (Hashemi et al., 2021).
iv.
RT-dPCR (Reverse Transcription Digital
Polymerase Chain Reaction)
SARS-CoV-2 RNA may be found and measured
using RT-dPCR, a sophisticated and extremely sensitive molecular diagnostic method.
By dividing the reaction into thousands of separate droplets or wells, RT-dPCR enables
absolute quantification of viral RNA, in contrast to conventional RT-qPCR, which
offers relative quantification. Each partition acts
as a microreactor containing either zero or one template molecule of the target
RNA. Following reverse transcription to cDNA and amplification through PCR, fluorescence
signals are measured for each partition to determine whether the target RNA is present.
This digital strategy has a number
of clear benefits. Particularly for samples with low viral loads or when the viral
RNA is degraded, it offers remarkable sensitivity and accuracy. The method is very
dependable for clinical diagnostics as it also reduces the impact of inhibitors
found in patient samples. Additionally, RT-dPCR is
less likely to be inconsistent, providing accurate data that are perfect for tracking
the dynamics of viral load over time, especially in prolonged COVID cases, or for
identifying leftover viral RNA after recovery (Suo et al., 2020).
RT-dPCR has been used
increasingly for SARS-CoV-2 research and diagnostic applications, such as determining
vaccination response, discovering new variations, and assessing treatment efficacy. Its drawbacks, such as increased expenses,
intricate procedures, and the requirement for specialist equipment, might prevent
the technology from being widely used in standard diagnostic settings (Shafie et al., 2023).
For high-precision viral RNA quantification, RT-dPCR is a potent technology that
offers substantial advantages in research and certain clinical applications, notwithstanding
these difficulties.
v.
Other Nucleic Acid Amplification Tests
(NAATs)
In addition to RT-qPCR
and RT-dPCR, several other NAAT colourgens have been designed for the identification
of SARS-CoV-2 (FDA, 2024). These techniques aim at increasing the usability, modularity
and productivity of diagnosis in various care and population health approaches.
A. Loop-Mediated Isothermal Amplification (LAMP):
LAMP is one of the quickest and least
expensive NAAT that doesn’t expect dynamic thermal cycling since it cycles the viral
RNA at a stationary temperature. The assay yields results within one hour using
specific primers and a strand-displacing DNA polymerase. For this reason, given
that these tests are easy to perform, require little equipment, and are highly sensitive,
they are very useful in low resource settings (CDC, 2023; Sagar et al., 2023).
Subsequently, to ease interpretation, several LAMP tests undergo further enhancements
utilizing colorimetric or fluorometric detection.
B. Transcription-Mediated
Amplification (TMA):
Another sensitive and accurate isothermal
system targeting SARS-CoV-2 RNA is TMA. It is particularly valuable in the high-throughput
testing and is associated with high sensitivity. TMA method can be used extensively
in labs and diagnostic centres since it is applied on automated platforms (Dierks
et al., 2021).
C. Clustered
Regularly Interspaced Short Palindromic Repeats (CRISPR)-Based Detection:
CRISPR has been adapted to identify SARS-CoV-2
by applying guide RNA sequences toward viral RNA. A measurable signal is generated
when CAS proteins – including Cas12 or Cas13 – bind to the target and activate and
digest the reporter (Deol et al., 2022). These assays are ideal candidates
for point-of-care testing because they are the following: rapid, adaptable, and
selective.
D. Helicase-Dependent
Amplification (HDA):
Primers may then attach and amplify DNA
or RNA using Helicase enzymes in HDA; an isothermal technique that unwinds DNA.
This kind of method is best used in field applications because of its simplicity
and compatibility with simple equipment (Zasada et al., 2022).
E. Nicking
Enzyme Amplification Reaction (NEAR):
Enzymes capable of nicking at specific
sites help to create single stranded DNA at that locations, NEAR is a very fast
nucleic acid amplification method that enables the polymerase to elongate the strand
for amplification. The NEAR-based assays are used in many portable diagnostic devices
since the results can be obtained in a very short time, in minutes (James et
al., 2020).
F. Rolling
Circle Amplification (RCA):
Standard Bacterial
DNAs are circularized and kept in checked throughout RCA, creating lengthy successive
sequences which may be identified through various methods. Other studies have shown
that RCA has high specificity and that it is useful when used in multiplex testing
but it is not as widely used as other NAATs. All these alternative NAATs offer the
following unique and valuable characteristics for SARS-CoV-2 related diagnostics:
versatility in terms of platforms, design, equipment, rapidity, and resource requirements
(Gu et al., 2018). Each of these methods involves its own optimizing factors
and constraints so that healthcare systems can select according to organizational
need.
vi.
Serological Tests
The existence of antibodies or
antigens in blood samples is detected by certain tests known as serological tests.
These tests are beneficial in analyzing the immunological reactions, identifying
the levels of immunities in a population and in identifying previous infections.
In particular, they complement the measurements based on nucleic acids for the detection
of immunological reactions to SARS-CoV-2 (CDC, 2023).
i.RAT
Rapid Antigen Tests
(RATs) are rapidly used for screening infected with SARS-CoV-2 antigens which are
portions of viral proteins in specimens such as nasal or throat swabs. Antigen tests
mainly use what is known as immunochromatographic assays whereby sample is applied
on a test device and in presence of the SARS-CoV-2 antigens, a visible signal is
generated. RATs have numerous benefits including; being fast with results taking
15-30 minutes, easy to use and inexpensive making them fit for use during mass screening
in the community, and at home. They are most useful for the quick identification
of persons who have a contagion; which is critical in preventing the spread of an
illness. However, their main drawback is suboptimal sensitivity when compared with
the increased specificity of other molecular techniques, including RT-PCR. This
implies that, compared to RT-PCR, RATs are inclined to deliver negative outcomes
even in persons who truly have COVID-19 but with low viral loads inclusive of asymptomatic
or early-stage patients (Sagar et al., 2023). In addition, reactions with
other coronaviruses or pathogens can lead to false-positive results, as such these
tests can be highly inaccurate at times. However, RATs are useful in high throughput
testing where speed is of essence, although follow up testing through more precise
techniques is advised.
ii.ELISA
Symptoms also have
limitations with tests like the PCR test, Antigen test and Enzyme-Linked Immunosorbent
Assay (ELISA) which are highly sensitive and specific laboratory tests that are
mostly used for the detection of covert antibodies against SARS-CoV-2. ELISA function
in that viral antigens or antibodies are attached to the surface of a plate and
then incubated in a medium and reacted with another reagent that produces color
change when the target antibodies or antigens are bound. This type of quantitative
test has more data outcomes compared to that of antigen tests that separate tests
of different antibodies such as IgM, IgG, and IgA that is representing of recent
infection and immunity levels. ELISA has been employed usefully in various large-scale
epidemiological surveys to identify seropositivity or effectiveness of immunization
and the amount of results is useful for a long-term antibody response evaluation.
Nonetheless, ELISA and other methods mentioned above have drawbacks as follows:
ELISA demands specific equipment and highly professional personnel; it requires
much greater reaction time, often measured in hours and days, compared to other
techniques, which makes it less appropriate for speedy point of care diagnostics.
Also, when comparing ELISA with other types of methods, it should be noted that
although this method allows determining the presence of antibodies in samples with
high specificity and sensitivity, this method can fail to detect viral infection
in patients during the acute phase of viral infection, when titter of detectable
antibodies is usually low or absent (Castellanos et al., 2022). Hence ELISA is best used in examining
samples collected after infection or after vaccination and not prognostically.
iii.Shortcomings of Antigen Tests
Shortcomings of
Antigen Tests are perhaps more observed when compared with the more accurate
nucleic acid amplification tests, (NAATs). Compared to antigen tests, PCR tests,
and antibody tests, there are many benefits to tests that use antigens: they are
fast and inexpensive, but they are less accurate when the viral load is low, as
occurs in asymptomatic patients or those who are beginning to recover from the virus.
The minimally derisked RATs enhance the prospects of false negative, a situation
which prolongs the time one has to isolating and therefore prolonging transmission.
Further, antigen tests are less informative and rarely give quantitative values
of viral loads or antibodies indicating severity of the disease or immunity respectively.
In addition, there are disadvantages in taking antigen tests which are the ability
in identifying the new variants of SARS-CoV-2 in cases there are mutations occur
in the viral proteins used in the tests. The fact is that the same antibodies associate
with other coronavirus strains, including those potentially causing colds, may give
a positive result, making diagnosis more challenging. These weaknesses explain why
antigen testing should be complemented by other diagnostics or confirmatory tests
when a negative test is given in patients with symptoms or outbreaks in high-incidence
areas. Consequently, such tests are less sensitive than more elaborate serologic
tests, such as ELISA or molecular tests, such as RT-PCR, even though the antigen
tests are relatively faster (Xin et al., 2021).
Molecular tests like
RATs and ELISA provide the diagnostic utility and information about immunity to
SARS-CoV-2 infection. This is the case since RATs are particularly useful in cases
of large-scale screening, avenues with a high population influx besides other large-scale
tests; albeit less sensitive than antigen tests. Compared to ELISA, it is more time
consuming and expensive, but offers information about the duration of immunity,
which is crucial for the epidemiological observation. However, there are some restrictions
of both tests which are important to consider while analysis the results (Johnson et al., 2022). When used alongside molecular testing
such as the RT-PCR these serological tools may prove useful in improving diagnostic
outcomes as well as assist the public health sectors in addressing COVID-19 pandemic.
4. Ancillary Tests for COVID-19
These additional tests
of COVID-19 give valuable information on the virus’s genome, mutation, and the immune
response to the disease other than basic diagnostic approaches like the RT-PCR and
antigen tests. The two key supplementary tests adopted in the detection and management
of COVID-19 are Sequencing and Antibody Serology Tests. These tests are central
to the characterization of the viral transmission dynamics, identification of emerging
strains, as well as antibody response upon recovery or upon vaccination.
i.Sequencing
Sequencing is a visually highly
sophisticated method for resolving the genetic map of SARS-CoV-2 viruses, allowing
researchers and clinicians to learn more about the pathogens. This test entails
identifying the sequence of all nucleotides which make up RNA in the virus’ genome.
There are two primary types of sequencing used in the context of COVID-19: WGS and
targeted sequencing. Sequencing in methods such as whole genome sequencing means
decoding all the 6 bases of the virus genome which gives detailed information regarding
the virus mutation and variability. This method is invaluable for surveillant viral
evolution and identifying new variants as well as mutations that could alter transmissibility,
disease severity, and vaccine effectiveness (El-Daly et al., 2024).
The sequencing efforts are most
relevant to new VOCs such as Delta and Omicron variants that emerged and proven
to have partial immune breakout and altered disease impact. Sequencing also enables
refinement of spike protein or other locations and showcase which mutations can
affect recall of vaccines or therapeutic entities. It also tracks transmission of
variants and offers epidemiological intelligence that shapes public health approaches
on variants and COVID-19 Surges. Although sequencing gives useful data, it has not
been applied to daily Covid-19 detection because it is time-consuming, expensive,
and not easy to perform. But it is essential for surveillance, studying the way
the virus spreads and its effect, as well as for the development of a vaccine and
antiviral plan (WHO, 2021).
ii.Antibody Serology Tests
Serology tests are used to diagnosis
an antibody in the blood which is an immunoglobulin produced by the body’s immune
system due to an infection such as COVID-19. These tests are meant to reveal the
presence of such proteins as IgM, IgG and IgA that arise at different periods of
an infection or after the administration of a vaccine. Detection of antibodies often
means that the person experienced and was infected by the virus in the past through
natural infection or vaccination, but the results can give some clue about the level
of immunity the person has against the virus.
There is no role for serological
testing in diagnosis of active SARS-CoV-2 disease as antibodies take several days
to weeks to become detectable. However, they are of greater value in the context
of the epidemiological investigations, such as the overall prevalence of COVID-19
antibodies in the given population, the evaluation of the immunogenicity following
the COVID-19 vaccine administration, as well as in the development of further public
health interventions. These tests are useful to determine a subject that may not
show any symptoms or had very mild symptoms that they never took seriously during
the pandemic.
Antibody testing is also used
in research especially in determining the longevity of protection concerning COVID-19
immunity as well as the effectiveness of vaccines against the virus. For example,
it can be used to assess which kind of vaccines are more likely to provoke an immune
response in the organism. Nevertheless, serology tests are not ideal for all other
forms of SARS-CoV-2; some forms may affect the immune response. However, antibody
detection does not preclude subsequent episodes because reinfection may occur, particularly
with the circulating strains that have mutations associated with immune escape (Dimech et al., 2024).
5. Treatment Strategies
Despite the spike
of the COVID-19 cases, different approaches in treatment have been invented to address
the impacts of SARS-CoV-2 virus. The distinctive therapeutic strategies include
the possibility of interaction with the virus (antiviral treatment), cytokine storm
inhibition (modulation of the immune response), and innate tissue regeneration and
immune reinforcement (stem cell therapy). Further below, we discuss these treatment
options in details.
i.Antiviral Therapy
Antiviral drugs are
used with the purpose of interfering with the replication of SARS-CoV-2, so that
the viral burden does not become too high in the body and therefore does not cause
severe and widespread COVID-19. These treatments are very important in the initial
phases of the infection because they can possibly lower the chance of serious illness
and hospitalization.
i.Remdesivir
Remdesivir is none specific antiviral
drug, which belong to class of RNA polymerase inhibitors and acts by blocking RNA
dependent RNA polymerase (RdRp) synthesis which is required for the RNA viruses
replication including SARS-CoV-2. This inhibition in actuality stops the process
of replication and limits the viral quantity that continues vying for tissue possession
within the body. Though initially invented to treat Ebola, remdesivir was later
used for the treatment of COVID-19 and received authorization as the first antiviral
for COVID-19 (Kalil et al., 2021).
Another clinical trial, which
has been conducted comparing the effectiveness of remdesivir among patients with
Covid-19, demonstrated that the drug was more efficient if it had been used in the
initial stage of the disease, during the first week after the beginning of symptoms
in particular. That is why its usage was said to have reduced time taken to recover,
mainly among the hospitalized patients with moderate symptoms, though its effect
on the mortality rates is still undeclared. Remdesivir is given intravenously and
is employed mainly on severely affected patients with COVID 19 that needs oxygen
to assist with their breathing but is not used in mild cases or patients with mild
symptoms who can take treatment at home. However the drug has some drawbacks, one
of which is possible renal toxicity and hence should not be administered to patients
with chronic kidney disease (Cao et al., 2023).
ii.Nirmatrelvir–Ritonavir (Paxlovid)
Paxlovid is a combination of
two antiviral drugs: nirmatrelvir, a protease inhibitor, and ritonavir, an pharmacokinetic
booster of nirmatrelvir because it selectively inhibits the liver enzymes that metabolize
the drug. Specifically, Nirmatrelvir work against SARS-CoV-2 main protease (Mpro)
enzyme which play vital role in replication process of the virus. This reshape at
the end of the polyproteins has been blocked by nirmatrelvir to prevent further
development and replication of the virus (Greasley et al., 2022; Takashita et al., 2022; Imai et al., 2023).
Paxlovid is a medicine that is
prescribed to patients with mild to moderate COVID symptoms with high risk of developing
severe form of the infection. Clinical trials have shown that Paxlovid provides
protection against hospitalization and deaths by nearly 88% if administered early
within five days of developing symptoms. However, computerized processing is contraindicated
in severe renal or hepatic impaired patients due to drug interaction with other
drugs especially those that are metabolized by the enzymes in the cytochrome P450
complex. Although Paxlovid has proven highly effective at reducing the risk of severe
disease, it does not appear to help patients who are already presenting severe symptoms
or those admitted to hospital with significant organ dysfunction (Perelson et al., 2023).
ii.Immunomodulators
Immunomodulation too
targets at controlling immune cascade overdrive to SARS-CoV-2 leading to occurrences
of cytokine storms, ARDS and multiple organ dysfunction syndrome. These therapies
aim directing the immune system to focus on elements that provoke inflammation thereby
enabling body to heal itself from the effects of the infection without having to
damage the tissues irreparably.
i.Baricitinib (JAK Inhibitor)
Baricitinib is an orally active
Janus kinase (JAK) inhibitor which inhibits the activity of JAK-STAT pathway is
known to activate the inflammatory cytokines. This inhibition reduces proinflammatory
cytokines in the levels like IL-6,and IL-1 βwhich are in the inflammatory cascade
of COVID-19 especially in severe cases. As JAK inhibitors, baricitinib decreases
inflammation that leads to lung injury and organ failure and puts patient at risk
of poor survival (Huang et al., 2022).
Baricitinib is indicated for
the treatment of COVID-19 in patients with moderate, severe or severe COVID-19 symptoms
who will likely require supplemental oxygen or mechanical ventilation. Randomized
controlled trials have shown that baricitinib as an adjunct therapy with corticosteroids
decreases the mortality and the risk to require invasive mechanical ventilation
in severe COVID-19 patients. But it can also lead to infections because it alters
the patient’s immune system, thus making proper monitoring crucial during treatment.
Furthermore, baricitinib is contraindicated in patients with active infection or
with past history of cancer, since the drug increases the risk of malignancy and
serious infection (Wolfe et al., 2022).
ii.Tocilizumab (IL-6 Inhibitor)
Tocilizumab is a monoclonal antibody
acting selectively on and blocking the IL-6 cytokine molecule, which is released
in excessive amounts during a cytokine storm. Increased levels of IL-6 are associated
with high inflammation, organ dysfunction, and poor outcome in COVID-19 infected
patients. As an ‘antagonist’ to the IL-6 receptor, tocilizumab works to decrease
inflammation and precludes the deterioration of certain organs like the lungs, heart
and kidneys in particular (Rezabakhsh et al., 2024; Zhang et al., 2020). Tocilizumab is usually administered to
those severe COVID-19 patients admitted to the hospital with elevated IL-6 levels
and who need oxygen or mechanical ventilation. It was established that adding tocilizumab
to the regimen of high steroid action has a better effect on the treatment of severe
COVID-19 cases, decreasing mortality rates and the risk of mechanical ventilation.
However, patients treated with tocilizumab should be regularly checked for infections
and gastrointestinal perforations and exhibit liver enzyme abnormalities (Lu et
al., 2024).
iii.Cell Therapy
Continued discussion
has been made on cell-based therapies as an option for critical COVID-19 patients
or those with organ injury or no response to conventional interventions. These therapies
aims to enhance the immune response mechanisms, treat molecular and tissue injuries
and promote healing from viral initiated organ failures.
i.T Cell Therapy
T cell therapy is based on administration
of T lymphocytes (T cell), which are among the components of adaptive immunity.
These are important in medicating virus infected cells in the body Deng et al.,
(2006). SARS-CoV-2 clearance by T cells is critical in COVID-19, but T cells are
exhausted in critically ill or immunocompromised patients. T cell therapy is the
process of augmenting the activity of T cells whether autologous T cells obtained
from the patient’s blood or allogeneic T cells from a donor, to increase the fight
or response to SARS-CoV-2.
The early experiments have indicated
that T cell therapy can have benefit in patients with the severe COVID-19, in particular,
those who have dangerous prolonged viral replication or immunocompromised condition.
This is shown to have an advantage of aiding the body reach a means to clear the
virus and avoid reinfection. However, T cell therapy is relatively new today, and
more efforts are required in order to establish the best administrations, the safety
as well as the efficacy of the therapy (Wang et al., 2023).
ii.Mesenchymal Stem Cell (MSC) Therapy
MSCs (Mesenchymal stem cells) are a type of partially
characterized multipotent cell population derived from mesodermal tissues possessing
tissue repair/ regeneration capabilities as well as immune regulation. MSCs release
molecules that have various effects including promoting tissue remodelling, reducing
inflammation and promoting healing of injured organs. This makes MSC therapy appealing
to patients with the severe COVID-19 related injuries like ARDS, myocarditis, or
affected liver and kidneys (Sengupta et al., 2020).
In human clinical trials MSC
treatment has demonstrated effectiveness in the amelioration of lung pathology and
inflammation as well as boosting tissue repair in COVID-19 patients who experience
severe pneumonia (Ringden et al., 2022). MSCs are generally given intravenously
and in evidence that they are useful in reconstructing damaged lung tissue, shortening
time on the ventilator, and increasing overall survival. However, the ongoing studies
have reported an immediate benefit of the MSC therapy and there is still so much
more to be learned regarding the safety issues, the way MSC therapy works, and the
long-term impact it has on COVID-19 (Dilogo et al., 2021).
6. Vaccines
i.Impact of Vaccines on Epidemiology
of COVID-19
The current COVID-19 approved
vaccines were designed primarily for the basic strain of SARS-CoV-2. For the vaccines,
the mRNA vaccine BNT162b2 (Pfizer BioNTech) was 95\% effective for preventing symptomatic
infections, and the protein subunit vaccine was 90\% effective in a study done among
participants. Efficacy against both hospitalization and death was near complete
for both vaccines. But due to high rates of mutation in SARS-CoV-2, newer strains
appeared which lead to so-called breakthrough cases. For instance, these mutation
possess the latitude to avoid the neutralizing antibodies like JN.1, which is featured
in the Omicron variant (Dunkle et al., 2022).
Essential to vaccine protection
are neutralizing antibody titres that, however, wane rapidly and this is why boosters
are required. A new mRNA booster for the Omicron XBB.1.5 variant has been endorsed
and does certainly enhance the neutralizing antibody titers against the new strains,
and hence assists in sustaining the protection. Likewise, the hospitalization and
death rates persist at constant levels in vaccinated populations to show that getting
vaccinated helps to prevent severe disease sequelae (Wang et al ., 2024).
The research has also demonstrated
that the proportion of patients more than seventy-five years old and individuals
with immunocompromising diseases rose during the Omicron wave; nevertheless, the
severity of COVID and mortality dropped thanks to the vaccine. This implies that
preventing measures are very important for quantifying the impact of COVID-19 in
high-risk populations (Kojima et al., 2023).
ii.Disparities in COVID-19 Response between
High-Income and Low-Income Countries
Resource-rich countries in the
developed world—say, the United States—were in a position not only financially and
infrastructurally to guarantee large-scale vaccination but also to do so where these
options have simply not existed for low-resource settings. Developed countries could
have huge COVID-19 vaccine inventories, put up large vaccination centres, and use
apps to administer vaccines. On the other hand, lower income country especially
those in Africa were shaded off due to financial enablers and poor health systems
(Zaoui et al., 2023).
To avoid this, COVAX has been
developed to distribute vaccines across the globe by the end of 2023 in 2 billion
doses to save many lives (Sign et al., 2024). However, there is still an issue of vaccine
bequeathal and transportation even in the low income countries after making arrangement
of acquiring vaccines. Some of these difficulties have been addressed by solutions
such as extension of vaccines to normal immunization schedules, and establishment
of mobile immunization stations. Non-governmental organizations (NGOs) also collaborate
with government in delivery of these vaccines to harder to reach areas (Med et al., 2023).
iii.Pfizer-BioNTech COVID-19 Vaccine (mRNA Vaccine)
Pfizer-BioNTech’s BNT162b2, introduced
in 2020, is an mRNA form of COVID-19 vaccine first to receive an emergency use authorization.
BioNTech’s Comirnaty works by using adapted mRNA to carry out the genetic plan of
the spike glycoprotein of SARS-CoV-2 and delivers it encapsulated in lipid nanoparticles.
Early large-scale outcomes exposed the vaccine to have 95% efficacy in stopping
symptomatic illness and no severe side effects. Efficacy was found to be reduced
gradually, which suggests that booster doses are required (Vogel et al., 2021).
They said that the vaccine has
great efficiency against some variants such as the Beta and the Delta, with approximately
90 % effectiveness in preventing hospitalization due to the virus but the efficacy
of the vaccine in preventing infection in the first place is lower and wanes over
time (Sahin et al., 2020). Research has also indicated that a booster dose
increases protection and that it protects especially against serious outcomes such
as hospitalization and death. The research show during the Omicron wave that the
booster lessened the effectiveness and substantially hindered developing severe
disease but had a comparatively lesser efficiency in preventing breakthrough symptomatic
infection. Though it weakens human body more than usual flu, it still afforded substantial
degree of safeguard against hospitalization and severe infection (Polack et al.,
2020).
To address new variants, Pfizer-BioNTech
come up with adapted vaccines, monovalent and bivalent targeting specific Omicron
subtypes (BA.1, BA.4/BA.5 and XBB.1.5). The variant-adapted vaccines demonstrated
increased immunogenicity compared to the primary titer, and bivalent boosters provided
further protection concerning severe diseases and hospitalization (Moreira et al., 2022).
The tolerability of the vaccine
is generally acceptable, although some severe side reactions have been noted even
though they are rare. This list comprises myocarditis especially in men, coagulation
disruptions such as CVT and thrombocytopenia. Nonetheless, the research indicates
that vaccine-associated myocarditis often seems to have a more favourable prognosis
for the patient than myocarditis with other origins (Martinelli et al., 2023).
The vaccine’s safety was comparable
to that observed in the general population in immunocompromised populations, including
transplant recipients, there were no reports of organ rejection or serious adverse
effects. This implies that, there is no harm with regard to increased risk associated
with immunization with patients with compromised immune systems.
iv.Novavax COVID-19 Vaccine (Protein Subunit Vaccine)
The NVX-CoV2373 (Novavax) is a recombinant
spike protein COVID-19 vaccine, developed with the Matrix-M adjuvant to promote
broad immune response (“Novavax and Serum
Institute of India Announce World Health Organization Grants Emergency Use Listing
for NVX-CoV2373 COVID-19 Vaccine - Dec 17, 2021). It has been proven very effective
in the prevention of COVID-19 disease from the clinical trials because it has overall
efficacy of about 89-90% and efficacy against its variants such as Alpha and Delta.
It also provided confidence about its ability to act as a booster shot as post-vaccination
antibody levels rose sharply against several SARS-CoV-2 variants (Hotez et al. 2022). The data from phase III trials
show that NVX-CoV2373 is relatively safe; only minor to moderate side effects such
as headache and pain at the injection site. Despite the myocarditis and pericarditis
side effects, the number was few than the other vaccines side effects. The vaccine
proved real-world efficacy, protection comparing to comparator vaccines depending
on variants, NVX-CoV2373 offered generally high protection (Hotez et al. 2022). The new version of the vaccine
is NVX-CoV2601 approved for booster dose use in the US and appears to protect against
the XBB.1.5 but more research is needed on its ongoing safety and effectiveness.
In general, the mainstay is Novavax’s vaccine, which provides an additional non-mRNA
way to prevent COVID-19, based on reputable data on its safety and effectiveness
(Heath et al., 2021).
Conclusions
Early on in the pandemic, the cooperation of scientists around the globe
made it possible to get a clear picture of this new coronavirus. Many new detection
techniques and treatment approaches have been developed new and made available thereafter
to help contain the spread and enhance management of COVID-19. While continuing
the research and controversial COVID-19 is no longer considered a pandemic by the
World Health Organisation. They further ensure continued and renewal of vaccines
and treatments to counter any new variants of SARS-CoV-2 which will make the current
endemicity of COVID-19 worse.
References
Agrawal
U., Azcoaga-Lorenzo A., Fagbamigbe A.F., Vasileiou E., Henery P., Simpson C.R.,
Stock S.J., Shah S.A., Robertson C., Woolhouse M., et al. Association between
multimorbidity and mortality in a cohort of patients admitted to hospital with
COVID-19 in Scotland. J. R. Soc. Med. 2021;115:22–30. doi:
10.1177/01410768211051715. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Ajaz S.,
McPhail M.J., Singh K.K., Mujib S., Trovato F.M., Napoli S., Agarwal K.
Mitochondrial metabolic manipulation by SARS-CoV-2 in peripheral blood
mononuclear cells of patients with COVID-19. Am. J. Physiol.-Cell Physiol.
2021;320:C57–C65. doi: 10.1152/ajpcell.00426.2020. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Akkiz H.
Implications of the novel mutations in the SARS-CoV-2 genome for transmission,
disease severity, and the vaccine development. Front. Med. 2021;8:636532. Doi:
10.3389/fmed.2021.636532. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Akkiz H.
Implications of the novel mutations in the SARS-CoV-2 genome for transmission,
disease severity, and the vaccine development. Front. Med. 2021;8:636532. Doi:
10.3389/fmed.2021.636532. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Ayoubkhani
D., Bosworth M.L., King S., Pouwels K.B., Glickman M., Nafilyan V., Zaccardi
F., Khunti K., Alwan N.A., Walker A.S. Risk of Long Covid in people infected
with SARS-CoV-2 after two doses of a COVID-19 vaccine: Community-based, matched
cohort study. medRxiv. 2022 Doi: 10.1101/2022.02.23.22271388. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Belser
J.A., Rota P.A., Tumpey T.M. Ocular tropism of respiratory viruses. Microbiol.
Mol. Biol. Rev. 2013;77:144–156. Doi: 10.1128/MMBR.00058-12. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Cao Z.,
Gao W., Bao H., Feng H., Mei S., Chen P., Gao Y., Cui Z., Zhang Q., Meng X., et
al. VV116 versus Nirmatrelvir–Ritonavir for Oral Treatment of COVID-19. N.
Engl. J. Med. 2023;388:406–417. Doi: 10.1056/NEJMoa2208822. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Carfì A.,
Bernabei R., Landi F. Persistent symptoms in patients after acute COVID-19.
JAMA. 2020;324:603–605. Doi: 10.1001/jama.2020.12603. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Castellanos
M., Somoza Á. Emerging clinically tested detection methods for COVID-19. FEBS
J. 2022;290:3089–3104. Doi: 10.1111/febs.16469. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
CDC. COVID
Data Tracker. Centers for Disease Control and Prevention. https://covid.cdc.gov/covid-data-tracker/#variant-proportions.
Centers
for Disease Control and Prevention Considerations for SARS-CoV-2 Antigen
Testing for Healthcare Providers Testing Individuals in the Community [Online]
[(accessed on 10 April 2024)];2023 Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html. [Ref list]
Channappanavar
R., Perlman S. Pathogenic human coronavirus infections: Causes and consequences
of cytokine storm and immunopathology. Semin. Immunopathol. 2017;39:529–539.
Doi: 10.1007/s00281-017-0629-x. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Chen C.,
Zhou Y., Wang D.W. SARS-CoV-2: A potential novel etiology of fulminant
myocarditis. Herz. 2020;45:230–232. Doi: 10.1007/s00059-020-04909-z. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Chen T. Fomites
and the COVID-19 Pandemic: An Evidence Review on Its Role in Viral
Transmission. National Collaborating Centre for Environmental Health;
Vancouver, BC, Canada: 2021. pp. 1–24. [Google Scholar][Ref list]
Chen Y.,
Zhu W., Han X., Chen M., Li X., Huang H., Zhang M., Wei R., Zhang H., Yang C.,
et al. How does the SARS-CoV-2 reinfection rate change over time? The global
evidence from systematic review and meta-analysis. BMC Infect. Dis.
2024;24:339. Doi: 10.1186/s12879-024-09225-z. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Chung, Y.-S.;
Lam, C.-Y.; Tan, P.-H.; Tsang, H.-F.; Wong, S.-C. C. Comprehensive Review of
COVID-19: Epidemiology, Pathogenesis, Advancement in Diagnostic and Detection
Techniques, and Post-Pandemic Treatment Strategies. International Journal of
Molecular Sciences 2024, 25 (15), 8155. https://doi.org/10.3390/ijms25158155.
Cortellessa
G., Stabile L., Arpino F., Faleiros D.E., Van Den Bos W., Morawska L., Buonanno
G. Close proximity risk assessment for SARS-CoV-2 infection. Sci. Total
Environ. 2021;794:148749. Doi: 10.1016/j.scitotenv.2021.148749. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Davis
H.E., Mccorkell L., Vogel J.M., Topol E.J. Long COVID: Major findings,
mechanisms and recommendations. Nat. Rev. Microbiol. 2023;21:133–146. Doi:
10.1038/s41579-022-00846-2. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Deng X.,
Hackbart M., Mettelman R.C., O’brien A., Mielech A.M., Yi G., Kao C.C., Baker
S.C. Coronavirus non-structural protein 15 mediates evasion of dsRNA sensors
and limits apoptosis in macrophages. Proc. Natl. Acad. Sci. USA.
2017;114:E4251–E4260. Doi: 10.1073/pnas.1618310114. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Denison
M.R., Graham R.L., Donaldson E.F., Eckerle L.D., Baric R.S. Coronaviruses: An
RNA proofreading machine regulates replication fidelity and diversity. RNA
Biol. 2011;8:270–279. Doi: 10.4161/rna.8.2.15013. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Deol P, Madhwal A, Sharma G, Kaushik R, Malik YS. CRISPR use
in diagnosis and therapy for COVID-19. Methods Microbiol. 2022;50:123-150. Doi:
10.1016/bs.mim.2022.03.002. Epub 2022 May 6. PMID: 38013928; PMCID: PMC9073596.
Dierks S, Bader O, Schwanbeck J, Groß U, Weig MS, Mese K,
Lugert R, Bohne W, Hahn A, Feltgen N, Torkieh S, Denker FR, Lauermann P, Storch
MW, Frickmann H, Zautner AE. Diagnosing SARS-CoV-2 with Antigen Testing,
Transcription-Mediated Amplification and Real-Time PCR. J Clin Med. 2021 May
29;10(11):2404. Doi: 10.3390/jcm10112404. PMID: 34072381; PMCID: PMC8199284.
Dilogo
I.H., Aditianingsih D., Sugiarto A., Burhan E., Damayanti T., Sitompul P.A.,
Mariana N., Antarianto R.D., Liem I.K., Kispa T., et al. Umbilical Cord
Mesenchymal Stromal Cells as Critical COVID-19 Adjuvant Therapy: A Randomized
Controlled Trial. Stem Cells Transl. Med. 2021;10:1279–1287. Doi:
10.1002/sctm.21-0046. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Dimech W.,
Curley S., Cai J.J. Comprehensive, comparative evaluation of 25 automated
SARS-CoV-2 serology assays. Microbiol. Spectr. 2024;12:e03228-23. Doi:
10.1128/spectrum.03228-23. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Dunkle
L.M., Kotloff K.L., Gay C.L., Áñez G., Adelglass J.M., Barrat Hernández A.Q.,
Harper W.L., Duncanson D.M., McArthur M.A., Florescu D.F., et al. Efficacy and
safety of NVX-CoV2373 in adults in the United States and Mexico. N. Engl. J.
Med. 2022;386:531–543. Doi: 10.1056/NEJMoa2116185. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
El-Daly
M.M. Advances and Challenges in SARS-CoV-2 Detection: A Review of Molecular and
Serological Technologies. Diagnostics. 2024;14:519. Doi:
10.3390/diagnostics14050519. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Fogarty
H., Townsend L., Morrin H., Ahmad A., Comerford C., Karampini E., Englert H.,
Byrne M., Bergin C., O’sullivan J.M., et al. Persistent endotheliopathy in the
pathogenesis of long COVID syndrome. J. Thromb. Haemost. 2021;19:2546–2553.
Doi: 10.1111/jth.15490. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Food and
Drug Administration At Home OTC COVID-19 Diagnostic Tests [Online] [(accessed
on 10 April 2024)];2024 Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/home-otc-covid-19-diagnostic-tests. [Ref list]
Food and
Drug Administration In Vitro Diagnostics EUAs—Molecular Diagnostic Tests for
SARS-CoV-2 [Online] [(accessed on 1 July 2024)];2024 Available online: https://www.fda.gov/medical-devices/covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-molecular-diagnostic-tests-sars-cov-2. [Ref list]
Food and
Drug Administration Novavax COVID-19 Vaccine, Adjuvanted [Online] [(accessed on
6 July 2024)];2023 Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/novavax-covid-19-vaccine-adjuvanted#additional. [Ref list]
Gao W., Lv
J., Pang Y., Li L.-M. Role of asymptomatic and pre-symptomatic infections in
COVID-19 pandemic. BMJ. 2021;375:n2342. Doi: 10.1136/bmj.n2342. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Greasley
S.E., Noell S., Plotnikova O., Ferre R., Liu W., Bolanos B., Fennell K., Nicki
J., Craig T., Zhu Y., et al. Structural basis for the in vitro efficacy of
nirmatrelvir against SARS-CoV-2 variants. J. Biol. Chem. 2022;298:101972. Doi:
10.1016/j.jbc.2022.101972. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Greenhalgh
T., Knight M., A’court C., Buxton M., Husain L. Management of post-acute
COVID-19 in primary care. BMJ. 2020;370:m3026. Doi: 10.1136/bmj.m3026. [DOI] [PubMed] [Google Scholar][Ref list]
Grobbelaar
L.M., Venter C., Vlok M., Ngoepe M., Laubscher G.J., Lourens P.J., Steenkamp
J., Kell D.B., Pretorius E. SARS-CoV-2 spike protein S1 induces fibrin (ogen)
resistant to fibrinolysis: Implications for microclot formation in COVID-19.
Biosci. Rep. 2021;41:BSR20210611. Doi: 10.1042/BSR20210611. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Gu, L., Yan, W., Liu, L., Wang, S., Zhang, X., & Lyu, M.
(2018). Research Progress on Rolling Circle Amplification (RCA)-Based
Biomedical Sensing. Pharmaceuticals, 11(2),
35. https://doi.org/10.3390/ph11020035
Gupta A.,
Madhavan M.V., Sehgal K., Nair N., Mahajan S., Sehrawat T.S., Bikdeli B.,
Ahluwalia N., Ausiello J.C., Wan E.Y., et al. Extrapulmonary manifestations of
COVID-19. Nat. Med. 2020;26:1017–1032. Doi: 10.1038/s41591-020-0968-3. [DOI] [PubMed] [Google Scholar][Ref list]
Haider N.,
Hasan M.N., Guitian J., Khan R.A., McCoy D., Ntoumi F., Dar O., Ansumana R.,
Uddin J., Zumla A., et al. The disproportionate case-fatality ratio of COVID-19
between countries with the highest vaccination rates and the rest of the world.
IJID Reg. 2023;6:159–166. Doi: 10.1016/j.ijregi.2023.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Hashemi
S.A., Safamanesh S., Ghasemzadeh-moghaddam H., Ghafouri M., Azimian A. High
prevalence of SARS-CoV-2 and influenza A virus (H1N1) coinfection in dead
patients in Northeastern Iran. J. Med. Virol. 2021;93:1008–1012. Doi:
10.1002/jmv.26364. [DOI] [PubMed] [Google Scholar][Ref list]
Heath
P.T., Galiza E.P., Baxter D.N., Boffito M., Browne D., Burns F., Chadwick D.R.,
Clark R., Cosgrove C., Galloway J., et al. Safety and efficacy of NVX-CoV2373
COVID-19 vaccine. N. Engl. J. Med. 2021;385:1172–1183. Doi:
10.1056/NEJMoa2107659. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list].
Horton, R.
Offline: 2019-nCoV outbreak—early lessons. The Lancet 2020, 395
(10221), 322. https://doi.org/10.1016/s0140-6736(20)30212-9.
Hotez
P.J., Bottazzi M.E. Whole inactivated virus and protein-based COVID-19
vaccines. Annu. Rev. Med. 2022;73:55–64. Doi:
10.1146/annurev-med-042420-113212. [DOI] [PubMed] [Google Scholar][Ref list]
Huang J.,
Zhou C., Deng J., Zhou J. JAK inhibition as a new treatment strategy for
patients with COVID-19. Biochem. Pharmacol. 2022;202:115162. Doi: 10.1016/j.bcp.2022.115162. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Imai M.,
Ito M., Kiso M., Yamayoshi S., Uraki R., Fukushi S., Watanabe S., Suzuki T.,
Maeda K., Sakai-Tagawa Y., et al. Efficacy of Antiviral Agents against Omicron
Subvariants BQ.1.1 and XBB. N. Engl. J. Med. 2023;388:89–91. Doi:
10.1056/NEJMc2214302. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
James AS, Alawneh JI. COVID-19 Infection Diagnosis: Potential
Impact of Isothermal Amplification Technology to Reduce Community Transmission
of SARS-CoV-2. Diagnostics (Basel). 2020 Jun 11;10(6):399. Doi:
10.3390/diagnostics10060399. PMID: 32545412; PMCID: PMC7345291.
Jiang S.,
Hillyer C., Du L. Neutralizing antibodies against SARS-CoV-2 and other human
coronaviruses. Trends Immunol. 2020;41:355–359. Doi: 10.1016/j.it.2020.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Johnson
B.A., Zhou Y., Lokugamage K.G., Vu M.N., Bopp N., Crocquet-Valdes P.A.,
Kalveram B., Schindewolf C., Liu Y., Scharton D., et al. Nucleocapsid mutations
in SARS-CoV-2 augment replication and pathogenesis. PLoS Pathog.
2022;18:e1010627. Doi: 10.1371/journal.ppat.1010627. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Kaku Y.,
Yo M.S., Tolentino J.E., Uriu K., Okumura K., Ito J., Sato K. Virological
characteristics of the SARS-CoV-2 KP. 3, LB. 1, and KP. 2.3 variants. Lancet
Infect. Dis. 2024 Doi: 10.1016/S1473-3099(24)00415-8. [DOI] [PubMed] [Google Scholar][Ref list]
Kalil
A.C., Mehta A.K., Patterson T.F., Erdmann N., Gomez C.A., Jain M.K., Wolfe
C.R., Ruiz-Palacios G.M., Kline S., Pineda J.R., et al. Efficacy of interferon
beta-1a plus remdesivir compared with remdesivir alone in hospitalised adults
with COVID-19: A double-blind, randomised, placebo-controlled, phase 3 trial.
Lancet Respir. Med. 2021;9:1365–1376. Doi: 10.1016/S2213-2600(21)00384-2. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Kojima N.,
Adams K., Self W.H., Gaglani M., McNeal T., Ghamande S., Steingrub J.S.,
Shapiro N.I., Duggal A., Busse L.W., et al. Changing severity and epidemiology
of adults hospitalized with coronavirus disease 2019 (COVID-19) in the United
States after introduction of COVID-19 vaccines, March 2021–August 2022. Clin.
Infect. Dis. 2023;77:547–557. Doi: 10.1093/cid/ciad276. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Lu D.-E.,
Ou T.-Y., Kang J.-W., Ong J.Y., Chen I.-J., Lee C.-H., Lee M.-C. The
association between tocilizumab and the secondary bloodstream infection maybe
nonsignificant in hospitalized patients with SARS-CoV-2 infection: A cohort
study. J. Microbiol. Immunol. Infect. 2024;57:38–47. Doi:
10.1016/j.jmii.2023.10.011. [DOI] [PubMed] [Google Scholar][Ref list]
Lu Q., Shi
Y. Coronavirus disease (COVID-19) and neonate: What neonatologist need to know.
J. Med. Virol. 2020;92:564–567. Doi: 10.1002/jmv.25740. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Ludwig, S.;
Zarbock, A. Coronaviruses and SARS-CoV-2: A Brief Overview. Anesthesia &
Analgesia 2020, 131 (1), 93–96. https://doi.org/10.1213/ane.0000000000004845.
Martinelli
S., Pascucci D., Laurenti P. Humoral response after a fourth dose of SARS-CoV-2
vaccine in immunocompromised patients. Results of a systematic review. Front.
Public Health. 2023;11:1108546. Doi: 10.3389/fpubh.2023.1108546. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Mccarthy
M.W. Metformin as a potential treatment for COVID-19. Expert Opin.
Pharmacother. 2023;24:1199–1203. Doi: 10.1080/14656566.2023.2215385. [DOI] [PubMed] [Google Scholar][Ref list]
Mccarthy
M.W. Paxlovid as a potential treatment for long COVID. Expert Opin.
Pharmacother. 2023;24:1839–1843. Doi: 10.1080/14656566.2023.2262387. [DOI] [PubMed] [Google Scholar][Ref list]
Med Aditus
Rwanda Welcomes Africa’s First Mobile Vaccine-Production Units. Med Aditus.
[Online] 2023. [(accessed on 30 June 2024)]. Available online: https://medaditus.org/news-articles/rwanda-welcomes-africas-first-mobile-vaccine-production-units/ [Ref list]
Mehta P.,
McAuley D.F., Brown M., Sanchez E., Tattersall R.S., Manson J.J., on behalf of
the HLH Across Speciality Collaboration, UK COVID-19: Consider cytokine storm
syndromes and immunosuppression. Lancet. 2020;395:1033–1034. Doi:
10.1016/S0140-6736(20)30628-0. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Mlcochova
P., Kemp S., Dhar M.S., Papa G., Meng B., Mishra S., Whittaker C., Mellan T.,
Ferreira I., Datir R., et al. SARS-CoV-2 B. 1.617. 2 Delta variant emergence,
replication and sensitivity to neutralising antibodies. BioRxiv. 2021 Doi:
10.1101/2021.05.08.443253. [DOI] [Google Scholar][Ref list]
Moreira
E.D., Kitchin N., Xu X., Dychter S.S., Lockhart S., Gurtman A., Perez J.L.,
Zerbini C., Dever M.E., Jennings T.W., et al. Safety and Efficacy of a Third
Dose of BNT162b2 COVID-19 Vaccine. N. Engl. J. Med. 2022;386:1910–1921. Doi:
10.1056/NEJMoa2200674. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Novavax
Novavax and Serum Institute of India Announce World Health Organization Grants
Emergency Use Listing for NVX-CoV2373 COVID-19 Vaccine [Online] 2021.
[(accessed on 6 July 2024)]. Available online: https://ir.novavax.com/press-releases/2021-12-17-Novavax-and-Serum-Institute-of-India-Announce-World-Health-Organization-Grants-Emergency-Use-Listing-for-NVX-CoV2373-COVID-19-Vaccine. [Ref list]
Novavax
Novavax Submits Application to U.S. FDA for Updated Protein-Based 2024–2025
Formula COVID-19 Vaccine [Online] 2024. [(accessed on 6 July 2024)]. Available
online: https://ir.novavax.com/press-releases/2024-06-14-Novavax-Submits-Application-to-U-S-FDA-for-Updated-Protein-based-2024-2025-Formula-COVID-19-Vaccine. [Ref list]
Ogimi, C.;
Kim, Y. J.; Martin, E. T.; Huh, H. J.; Chiu, C.-H.; Englund, J. A. What’s New
With the Old Coronaviruses? Journal of the Pediatric Infectious Diseases
Society 2020, 9 (2), 210–217. https://doi.org/10.1093/jpids/piaa037.
Peiris, J.;
Lai, S.; Poon, L.; Guan, Y.; Yam, L.; Lim, W.; Nicholls, J.; Yee, W.; Yan, W.;
Cheung, M.; Cheng, V.; Chan, K.; Tsang, D.; Yung, R.; Ng, T.; Yuen, K.
Coronavirus as a possible cause of severe acute respiratory syndrome. The
Lancet 2003, 361 (9366), 1319–1325. https://doi.org/10.1016/s0140-6736(03)13077-2.
Perelson
A.S., Ribeiro R.M., Phan T. An explanation for SARS-CoV-2 rebound after
Paxlovid treatment. medRxiv. 2023 Doi: 10.1101/2023.05.30.23290747. [DOI] [Google Scholar][Ref list]
Planas D.,
Staropoli I., Michel V., Lemoine F., Donati F., Prot M., Porrot F.,
Guivel-Benhassine F., Jeyarajah B., Brisebarre A., et al. Distinct evolution of
SARS-CoV-2 Omicron XBB and BA.2.86/JN.1 lineages combining increased fitness
and antibody evasion. Nat. Commun. 2024;15:2254. Doi:
10.1038/s41467-024-46490-7. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Polack
F.P., Thomas S.J., Kitchin N., Absalon J., Gurtman A., Lockhart S., Perez J.L.,
Pérez Marc G., Moreira E.D., Zerbini C., et al. Safety and efficacy of the
BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020;383:2603–2615. Doi:
10.1056/NEJMoa2034577. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Pulliam
J.R., van Schalkwyk C., Govender N., von Gottberg A., Cohen C., Groome M.J.,
Dushoff J., Mlisana K., Moultrie H. Increased risk of SARS-CoV-2 reinfection
associated with emergence of Omicron in South Africa. Science.
2022;376:eabn4947. Doi: 10.1126/science.abn4947. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Ravindra
K., Malik V., Padhi B., Goel S., Gupta M. Asymptomatic infection and
transmission of COVID-19 among clusters: Systematic review and meta-analysis.
Public Health. 2021;203:100–109. Doi: 10.1016/j.puhe.2021.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Rezabakhsh
A., Mojtahedi F., Tekantapeh S.T., Mahmoodpoor A., Ala A., Soleimanpour H.
Therapeutic Impact of Tocilizumab in the Setting of Severe COVID-19; an Updated
and Comprehensive Review on Current Evidence. Arch. Acad. Emerg. Med.
2024;12:e47. Doi: 10.22037/aaem.v12i1.2217. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Ringden
O., Roshandel E., Pirsalehi A., Kazemi S., Sankanian G., Majidi M., Salimi M.,
Aghdami N., Sadrosadat H., Kochaksaraei S.S., et al. Conquering the cytokine
storm in COVID-19-induced ARDS using placenta-derived decidua stromal cells.
Biol. Blood Marrow Transplant. 2022;28:S222. Doi:
10.1016/S2666-6367(22)00440-7. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Rodriguez
H., Hartert T.V., Gebretsadik T., Carroll K.N., Larkin E.K. A simple
respiratory severity score that may be used in evaluation of acute respiratory
infection. BMC Res. Notes. 2016;9:1–4. Doi: 10.1186/s13104-016-1899-4. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Sagar, V., Singh, M. P., Kaur, G., Khurana, R., Agarwal, R.,
Ratho, R. K., Ghosh, A., Kulashri, A., & Aggarwal, A. K. (2023). LAMP-Based
Point-of-Care Nucleic Acid-Based Detection Method Can Be Useful for Quick
Decision-Making for Diagnosis of Acute COVID-19 Emergency Cases in Hospital
Settings. COVID,
3(6),
914-923. https://doi.org/10.3390/covid3060066
Sahin U.,
Muik A., Derhovanessian E., Vogler I., Kranz L.M., Vormehr M., Baum A., Pascal
K., Quandt J., Maurus D., et al. COVID-19 vaccine BNT162b1 elicits human
antibody and TH1 T-cell responses. Nature. 2020;586:594–599. Doi:
10.1038/s41586-020-2814-7. [DOI] [PubMed] [Google Scholar][Ref list]
Sengupta
V., Sengupta S., Lazo A., Woods P., Nolan A., Bremer N. Exosomes Derived from
Bone Marrow Mesenchymal Stem Cells as Treatment for Severe COVID-19. Stem Cells
Dev. 2020;29:747–754. Doi: 10.1089/scd.2020.0080. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Shafie
M.H., Antony Dass M., Ahmad Shaberi H.S., Zafarina Z. Screening and
confirmation tests for SARS-CoV-2: Benefits and drawbacks. Beni Suef Univ. J.
Basic Appl. Sci. 2023;12:6. Doi: 10.1186/s43088-023-00342-3. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Sign¢ L.
Strategies for Effective Health Care for Africa in the Fourth Industrial
Revolution, Bridging the Gap between the Promise and Delivery. [Online] 2021.
[(accessed on 2 July 2024)]. Available online: https://www.brookings.edu/wp-content/uploads/2021/10/Strategies-for-effective-health-care-delivery-in-Africa_FINAL.pdf. [Ref list]
Singh I.,
Joseph P., Heerdt P.M., Cullinan M., Lutchmansingh D.D., Gulati M., Possick
J.D., Systrom D.M., Waxman A.B. Persistent exertional intolerance after
COVID-19: Insights from invasive cardiopulmonary exercise testing. Chest.
2022;161:54–63. Doi: 10.1016/j.chest.2021.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Singh
M.K., Mobeen A., Chandra A., Joshi S., Ramachandran S. A meta-analysis of
comorbidities in COVID-19: Which diseases increase the susceptibility of
SARS-CoV-2 infection? Comput. Biol. Med. 2021;130:104219. Doi:
10.1016/j.compbiomed.2021.104219. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Stertman
L., Palm A.K., Zarnegar B., Carow B., Lunderius Andersson C., Magnusson S.E.,
Carnrot C., Shinde V., Smith G., Glenn G., et al. The Matrix-M™ adjuvant: A
critical component of vaccines for the 21st century. Hum. Vaccines Immunother.
2023;19:2189885. Doi: 10.1080/21645515.2023.2189885. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Suo T.,
Liu X., Feng J., Guo M., Hu W., Guo D., Ullah H., Yang Y., Zhang Q., Wang X.,
et al. ddPCR: A more accurate tool for SARS-CoV-2 detection in low viral load
specimens. Emerg. Microbes Infect. 2020;9:1259–1268. Doi:
10.1080/22221751.2020.1772678. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Takashita
E., Yamayoshi S., Simon V., van Bakel H., Sordillo E.M., Pekosz A., Fukushi S.,
Suzuki T., Maeda K., Halfmann P., et al. Efficacy of Antibodies and Antiviral
Drugs against Omicron BA.2.12.1, BA.4, and BA.5 Subvariants. N. Engl. J. Med.
2022;387:468–470. Doi: 10.1056/NEJMc2207519. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Tsang, H. F.;
Chan, L. W. C.; Cho, W. C. S.; Yu, A. C. S.; Yim, A. K. Y.; Chan, A. K. C.; Ng,
L. P. W.; Wong, Y. K. E.; Pei, X. M.; Li, M. J. W.; Wong, S.-C. C. An update on
COVID-19 pandemic: the epidemiology, pathogenesis, prevention and treatment
strategies. Expert Review of Anti-infective Therapy 2020, 19
(7), 877–888. https://doi.org/10.1080/14787210.2021.1863146.
Vaira
L.A., Hopkins C., Sandison A., Manca A., Machouchas N., Turilli D., Lechien
J.R., Barillari M.R., Salzano G., Cossu A., et al. Olfactory epithelium
histopathological findings in long-term coronavirus disease 2019 related
anosmia. J. Laryngol. Otol. 2020;134:1123–1127. Doi: 10.1017/S0022215120002455. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
van Kampen
J.J., van de Vijver D.A., Fraaij P.L., Haagmans B.L., Lamers M.M., Okba N., van
den Akker J.P., Endeman H., Gommers D.A., Cornelissen J.J., et al. Duration and
key determinants of infectious virus shedding in hospitalized patients with
coronavirus disease-2019 (COVID-19) Nat. Commun. 2021;12:267. Doi: 10.1038/s41467-020-20568-4. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Vetter P.,
Eberhardt C.S., Meyer B., Murillo P.A.M., Torriani G., Pigny F., Lemeille S.,
Cordey S., Laubscher F., Vu D.-L., et al. Daily viral kinetics and innate and
adaptive immune response assessment in COVID-19: A case series. mSphere.
2020;5:e00827-20. Doi: 10.1128/mSphere.00827-20. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Vogel
A.B., Kanevsky I., Che Y., Swanson K.A., Muik A., Vormehr M., Kranz L.M.,
Walzer K.C., Hein S., Güler A., et al. BNT162b vaccines protect rhesus macaques
from SARS-CoV-2. Nature. 2021;592:283–289. Doi: 10.1038/s41586-021-03275-y. [DOI] [PubMed] [Google Scholar][Ref list]
Wang Q.,
Guo Y., Bowen A., Mellis I.A., Valdez R., Gherasim C., Gordon A., Liu L., Ho
D.D. XBB.1.5 monovalent mRNA vaccine booster elicits robust neutralizing
antibodies against XBB subvariants and JN.1. Cell Host Microbe. 2024;32:315–321.
Doi: 10.1016/j.chom.2024.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Wang Y.,
Liang Q., Chen F., Zheng J., Chen Y., Chen Z., Li R., Li X. Immune-Cell-Based
Therapy for COVID-19: Current Status. Viruses. 2023;15:2148. Doi:
10.3390/v15112148. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Watanabe
A., Iwagami M., Yasuhara J., Takagi H., Kuno T. Protective effect of COVID-19
vaccination against long COVID syndrome: A systematic review and meta-analysis.
Vaccine. 2023;41:1783–1790. Doi: 10.1016/j.vaccine.2023.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Wolfe
C.R., Tomashek K.M., Patterson T.F., Gomez C.A., Marconi V.C., Jain M.K., Yang
O.O., Paules C.I., Palacios G.M.R., Grossberg R., et al. Baricitinib versus
dexamethasone for adults hospitalised with COVID-19 (ACTT-4): A randomised,
double-blind, double placebo-controlled trial. Lancet Respir. Med.
2022;10:888–899. Doi: 10.1016/S2213-2600(22)00088-1. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Woo, P. C. Y.;
Lau, S. K. P.; Huang, Y.; Yuen, K.-Y. Coronavirus Diversity, Phylogeny and
Interspecies Jumping. Experimental Biology and Medicine 2009, 234
(10), 1117–1127. https://doi.org/10.3181/0903-mr-94.
World
Health Organization Coronavirus Disease (COVID-19) Situation Reports. [Online].
World Health Organization. 2024. [(accessed on 4 December 2024)]. Available
online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports. [Ref list]
World
Health Organization Genomic Sequencing of SARS-CoV-2: A Guide to Implementation
for Maximum Impact on Public Health. 8 January 2021. [(accessed on 24 July
2024)]. Available online: https://www.who.int/publications/i/item/9789240018440. [Ref list]
World
Health Organization Statement on the Fifteenth Meeting of the IHR (2005)
Emergency Committee on the COVID-19 Pandemic. [Online]. World Health
Organization. 2023. [(accessed on 26 June 2024)]. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic. [Ref list]
World
Health Organization Statement on the Update of Who’s Working Definitions and
Tracking System for SARS-COV-2 Variants of Concern and Variants of Interest.
[Online]. World Health Organization. 2023. [(accessed on 26 June 2024)].
Available online: https://www.who.int/news/item/16-03-2023-statement-on-the-update-of-who-s-working-definitions-and-tracking-system-for-sars-cov-2-variants-of-concern-and-variants-of-interest. [Ref list]
World
Health Organization Statement on the Update of Who’s Working Definitions and
Tracking System for SARS-COV-2 Variants of Concern and Variants of Interest.
[Online]. World Health Organization. 2023. [(accessed on 26 June 2024)].
Available online: https://www.who.int/news/item/16-03-2023-statement-on-the-update-of-who-s-working-definitions-and-tracking-system-for-sars-cov-2-variants-of-concern-and-variants-of-interest. [Ref list]
World
Health Organization Why Is COVID-19 Data Being Presented as Weekly Statistics?
[Online]. World Health Organization. 2024. [(accessed on 4th
December 2024)]. Available online: https://data.who.int/dashboards/covid19/cases?m49=156&n=c. [Ref list]
Wu D., Wu
T., Liu Q., Yang Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis.
2020;94:44–48. Doi: 10.1016/j.ijid.2020.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Wu J.,
Deng W., Li S., Yang X. Advances in research on ACE2 as a receptor for
2019-nCoV. Cell. Mol. Life Sci. 2020;78:531–544. Doi:
10.1007/s00018-020-03611-x. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Xin H., Li
Y., Wu P., Li Z., Lau E.H.Y., Qin Y., Wang L., Cowling B.J., Tsang T.K., Li Z.
Estimating the Latent Period of Coronavirus Disease 2019 (COVID-19) Clin.
Infect. Dis. 2021;74:1678–1681. Doi: 10.1093/cid/ciab746. [DOI] [PubMed] [Google Scholar][Ref list]
Zaoui S.,
Foguem C., Tchuente D., Fosso-Wamba S., Kamsu-Foguem B. The viability of supply
chains with interpretable learning systems: The case of COVID-19 vaccine
deliveries. Glob. J. Flex. Syst. Manag. 2023;24:633–657. Doi:
10.1007/s40171-023-00357-w. [DOI] [Google Scholar][Ref list]
Zasada AA, Mosiej E, Prygiel M, Polak M, Wdowiak K, Formińska
K, Ziółkowski R, Żukowski K, Marchlewicz K, Nowiński A, Nowińska J, Rastawicki
W, Malinowska E. Detection of SARS-CoV-2 Using Reverse Transcription Helicase
Dependent Amplification and Reverse Transcription Loop-Mediated Amplification
Combined with Lateral Flow Assay. Biomedicines. 2022 Sep 19;10(9):2329. Doi:
10.3390/biomedicines10092329. PMID: 36140431; PMCID: PMC9496027.
Zhang C.,
Wu Z., Li J.-W., Zhao H., Wang G.Q. The cytokine release syndrome (CRS) of
severe COVID-19 and Interleukin-6 receptor (IL-6R) antagonist Tocilizumab may
be the key to reduce the mortality. Int. J. Antimicrob. Agents. 2020;55:105954.
Doi: 10.1016/j.ijantimicag.2020.105954. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
Zimmerman
K. RECOVER-AUTONOMIC: A Platform Protocol for Evaluation of Interventions for
Autonomic Dysfunction in Post-Acute Sequelae of SARS-CoV-2 Infection (PASC).
[Online] 2024. [(accessed on 30 June 2024)]. Available online: https://trials.recovercovid.org/documents/RECOVER_AUTONOMIC_Protocol_V3.0.pdf. [Ref list]
Zohar T.,
Alter G. Dissecting antibody-mediated protection against SARS-CoV-2. Nat. Rev.
Immunol. 2020;20:392–394. Doi: 10.1038/s41577-020-0359-5. [DOI] [PMC free article] [PubMed] [Google Scholar][Ref list]
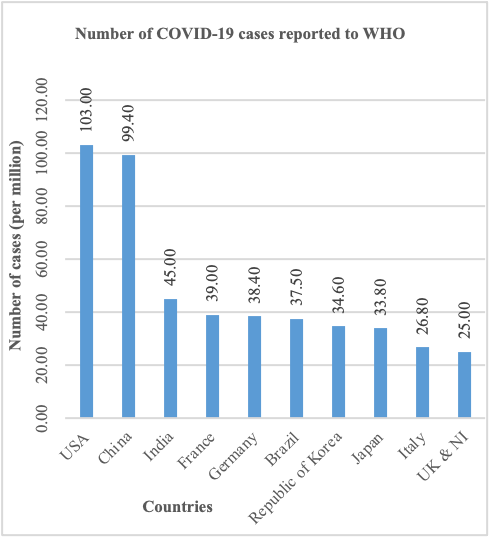 The COVID-19 can be traced from
the last quarter of December 2019 when a number of pneumonia cases of unknown causes
surfaced in Wuhan city, Hubei province, People’s Republic of China. The first few
cases were reported to be associated with the Huanan Wet Seafood Wholesale Market,
which sale live animals such as bats and snakes and thus pointed to possibility
of zoonotic transmission. First, the outbreak was believed to be caused by viral
pneumonia and further studies pointed out that the culprit is the novel coronavirus,
now known as SARS-CoV-2 because of its genetic and phylogenetic relationship with
SARS-CoV which caused the 2002/2003 SARS epidemic (Ludwig et al 2020). When studying SARS-CoV-2, researchers assumed that it also spread from
animals, and the contact with wildlife or consumption of animals could be the ways
of transmission. This prompted the Chinese authorities to close wet markets considered
unsanitary undertaking that constituted an initial measure to curb the epidemic
(Horton et al., 2020). However, the virus remained widespread and went
from one being contained in specific geographical regions to being a worldwide pandemic.
The COVID-19 can be traced from
the last quarter of December 2019 when a number of pneumonia cases of unknown causes
surfaced in Wuhan city, Hubei province, People’s Republic of China. The first few
cases were reported to be associated with the Huanan Wet Seafood Wholesale Market,
which sale live animals such as bats and snakes and thus pointed to possibility
of zoonotic transmission. First, the outbreak was believed to be caused by viral
pneumonia and further studies pointed out that the culprit is the novel coronavirus,
now known as SARS-CoV-2 because of its genetic and phylogenetic relationship with
SARS-CoV which caused the 2002/2003 SARS epidemic (Ludwig et al 2020). When studying SARS-CoV-2, researchers assumed that it also spread from
animals, and the contact with wildlife or consumption of animals could be the ways
of transmission. This prompted the Chinese authorities to close wet markets considered
unsanitary undertaking that constituted an initial measure to curb the epidemic
(Horton et al., 2020). However, the virus remained widespread and went
from one being contained in specific geographical regions to being a worldwide pandemic.